Non-Operative Management of Perforated Peptic Ulcer Disease: Outcomes and Evidence Review
-
Moses Adondua Abah

Department of Biochemistry, Faculty of Biosciences, Federal University Wukari, Taraba State, Nigeria
Onyinye Ifeoma IkedionwuDepartment of Medicine and Surgery, College of Medicine, University of Lagos, Idi-Araba, Lagos State, Nigeria
Obagade Ibukunoluwa OluwatoyinDepartment of Medicine and Surgery, College of Medicine, University of Lagos, Idi-Araba, Lagos State, Nigeria
Praise Udoka OputaDepartment of Medicine and Surgery, College of Medicine, University of Lagos, Idi-Araba, Lagos State, Nigeria
Jemiseye Abayomi VictorDepartment of Medicine and Surgery, College of Medicine, University of Lagos, Idi-Araba, Lagos State, Nigeria
Ezeudu Paschal ChikelumDepartment of Medicine and Surgery, College of Medicine, University of Lagos, Idi-Araba, Lagos State, Nigeria
| Received 23 Aug, 2025 |
Accepted 06 Oct, 2025 |
Published 10 Oct, 2025 |
Perforated Peptic Ulcer Disease (PPUD) is a serious complication traditionally managed surgically. With advances in supportive care, non-operative management (NOM) has emerged as a promising alternative for select patients. This review synthesizes evidence from observational studies, clinical trials, and case reports to evaluate the outcomes, safety, and limitations of NOM in PPUD. Conservative treatment typically involves intravenous antibiotics, proton pump inhibitors, nasogastric decompression, and close clinical monitoring. The NOM is generally suitable for hemodynamically stable patients without generalized peritonitis or sepsis and with localized perforations confirmed by imaging. Reported success rates range from 40-80%, with reduced morbidity, shorter hospitalization, and lower healthcare costs compared to surgery. Imaging, particularly CT scans, is crucial for diagnosis and monitoring. However, risk of failure increases with delayed presentation, large perforations, or malignancy, and mortality is higher when surgery is delayed after failed NOM. These findings underscore the importance of cautious patient selection, multidisciplinary care, and timely surgical conversion when indicated. While surgery remains essential in complicated cases, NOM offers a safe alternative for selected patients. Future randomized controlled trials are needed to establish standardized protocols and improve prognostic tools for patient stratification.
| Copyright © 2025 Abah et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Peptic Ulcer Disease (PUD) represents a significant gastrointestinal pathology characterized by the erosion of the mucosal lining of the stomach or duodenum, primarily due to the aggressive action of gastric acid and pepsin1. A critical and potentially life-threatening complication of PUD is perforation, where an ulcer breaches the gastrointestinal wall, resulting in the leakage of gastric or duodenal contents into the peritoneal cavity2. This event can precipitate acute peritonitis, Systemic Inflammatory Response Syndrome (SIRS), sepsis, and even death if not managed appropriately and promptly. Traditionally, the standard of care for Perforated Peptic Ulcer Disease (PPUD) has been surgical intervention, typically involving closure of the perforation via open or laparoscopic methods, along with thorough peritoneal lavage to mitigate contamination and infection3. However, evolving medical practice, advances in diagnostics, and better understanding of ulcer pathophysiology have facilitated a paradigm shift towards conservative, non-operative management (NOM) in selected patient populations4.
Non-operative management of PPUD is grounded in the principle of avoiding surgical risks in patients who may respond well to medical therapy alone5. This strategy typically includes aggressive resuscitation, Nil Per OS (NPO) status, nasogastric decompression, intravenous Proton Pump Inhibitors (PPIs), broad-spectrum antibiotics, and close clinical observation6. The growing body of literature supporting NOM arises from observations that some patients with contained or sealed perforations can recover without operative intervention, particularly those with stable vital signs, minimal peritoneal signs, and no evidence of diffuse peritonitis or sepsis7. The integration of computed tomography (CT) imaging with oral contrast has significantly enhanced the ability to distinguish between free perforations and those that are localized or sealed by adjacent organs or inflammatory adhesions. This has expanded the criteria for selecting patients suitable for conservative therapy. The rationale behind non-operative management is multifaceted8. Firstly, not all cases of PPUD are alike; while some perforations lead to catastrophic contamination and rapid deterioration, others may be small and effectively sealed by surrounding tissues, rendering them amenable to medical therapy. Secondly, surgery carries inherent risks, particularly in elderly or comorbid patients. Operative mortality rates can range from 6 to 30% depending on factors such as age, delay in presentation, physiological derangement, and the extent of peritoneal contamination9. In contrast, NOM may offer a less invasive and potentially safer alternative, especially in patients who meet well-defined criteria. Furthermore, advancements in antimicrobial therapy, acid suppression, and supportive care have enhanced the efficacy and safety of medical management protocols10.
Despite the growing interest and reported success in NOM, the practice remains controversial. Critics argue that delayed surgical intervention in patients who fail conservative therapy may result in worse outcomes due to prolonged peritoneal soiling, worsening sepsis, and increased operative difficulty11. Therefore, the success of NOM hinges on careful patient selection, stringent monitoring, and clear criteria for timely surgical conversion. Moreover, there is an ongoing debate regarding the reliability of imaging modalities to conclusively determine perforation status and the threshold at which NOM should be abandoned in favor of operative treatment. The literature presents mixed findings regarding outcomes of non-operative management. Several retrospective and prospective studies have reported favorable results in well-selected patients, with success rates ranging from 70 to 90%12. These studies have identified several predictors of successful NOM, including younger age, absence of shock, limited peritoneal signs, stable laboratory parameters, and minimal or localized pneumoperitoneum on imaging. On the other hand, failed conservative therapy can result in delayed surgery, longer hospital stays, higher morbidity, and increased healthcare costs13. Consequently, defining clear selection criteria and management protocols is critical to optimizing outcomes.
Historically, the shift toward non-operative strategies in the treatment of intra-abdominal pathologies has mirrored broader trends in surgical practice. Just as uncomplicated appendicitis and diverticulitis have seen increasing rates of conservative management, so too has PPUD been reevaluated in the light of less invasive strategies14. The seminal work in the 1980s identified prognostic factors (such as shock, comorbid disease, and delay in presentation) that remain relevant in guiding therapeutic decisions today. In modern times, scoring systems such as the Boey score, Mannheim peritonitis index, and American Society of Anesthesiologists (ASA) classification have been used to stratify risk and guide treatment strategies15.
Recent systematic reviews and meta-analyses have attempted to synthesize the available evidence on non-operative versus operative management, with varying conclusions. Some suggest that NOM is comparable to surgery in carefully selected cases, while others caution against its widespread adoption without further high-quality Randomized Controlled Trials (RCTs)16. The scarcity of RCTs in this domain is due in part to ethical challenges, the heterogeneity of clinical presentations, and variability in institutional protocols. Nevertheless, observational studies and real-world clinical experiences continue to provide valuable insights into the feasibility and safety of NOM17. In addition to clinical outcomes such as mortality, morbidity, length of hospital stay, and need for surgical conversion, quality of life and economic implications are also important considerations. Non-operative management, if successful, may reduce the burden of surgical recovery, lower healthcare costs, and improve patient satisfaction. However, this must be balanced against the risks of missed or delayed operative indications, which may exacerbate morbidity and prolong hospitalization18. Understanding the factors influencing these outcomes is crucial for clinicians to make informed decisions and for health systems to develop standardized protocols.
While surgical intervention remains the cornerstone of treatment for many cases of PPUD, non-operative management has emerged as a viable alternative in selected patients19. The success of this approach relies on accurate diagnosis, judicious patient selection, and close monitoring. As healthcare systems continue to evolve towards more personalized and less invasive care, understanding the outcomes and limitations of NOM is critical. Through this comprehensive review, we seek to elucidate the role of non-operative management in PPUD and contribute to the development of evidence-based guidelines that support safe, effective, and patient-centered care20.
This review aims to provide a comprehensive synthesis of the current evidence surrounding the outcomes of non-operative management of PPUD. It will explore patient selection criteria, clinical and radiological assessment, therapeutic strategies, and predictors of success or failure. The review will also compare outcomes of NOM with those of surgical management, highlight the limitations of existing studies, and identify areas for future research. Ultimately, the goal is to offer a balanced perspective on the role of non-operative management in the modern treatment algorithm of perforated peptic ulcer disease, helping clinicians navigate the complex interplay between patient safety, clinical efficacy, and resource optimization.
Etiology of peptic ulcers: Peptic Ulcer Disease (PUD) refers to the development of open sores or lesions in the lining of the stomach, duodenum or sometimes the lower esophagus21. The primary causes of peptic ulcers include.
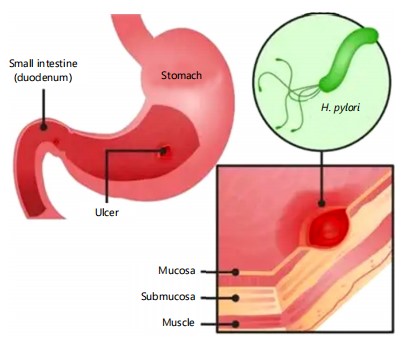
Helicobacter pylori: Helicobacter pylori (H. pylori) infection is the most common cause of peptic ulcers worldwide, particularly in the developing world22. This gram-negative, spiral-shaped bacterium colonizes the gastric mucosa, primarily in the antrum, and disrupts normal gastric defenses through multiple mechanisms. It produces the enzyme urease, which converts urea into ammonia, neutralizing stomach acid locally and enabling its survival in the acidic environment. The resulting alkaline microenvironment, combined with bacterial cytotoxins such as CagA and VacA, leads to mucosal inflammation, epithelial cell damage, and impaired mucosal healing23 (Fig. 1).
Chronic H. pylori infection promotes persistent gastritis, which weakens the mucosal barrier and makes it more susceptible to acid-peptic injury. Over time, this inflammation can lead to erosion of the mucosa, ulceration, and sometimes bleeding or perforation. The bacterium also stimulates increased gastrin production, which raises acid secretion, particularly in duodenal ulcers24. Transmission is primarily fecal-oral or oral-oral, and infection is often acquired during childhood. Not all infected individuals develop ulcers, indicating a role for host factors, bacterial virulence, and environmental conditions in ulcer development. Eradication of H. pylori with antibiotic therapy significantly reduces ulcer recurrence, underscoring its central role in peptic ulcer disease etiology25.
Figure 1 explains how H. pylori is a bacterium that colonizes the stomach lining and plays a major role in peptic ulcer disease. It produces urease, which neutralizes gastric acid, allowing it to survive in the acidic environment. The organism releases toxins and stimulates chronic inflammation, which weakens the protective mucosal barrier. This results in increased gastric acid damage, erosion of the stomach or duodenal lining, and formation of ulcers, often associated with abdominal pain, nausea, and complications like bleeding.
|
|
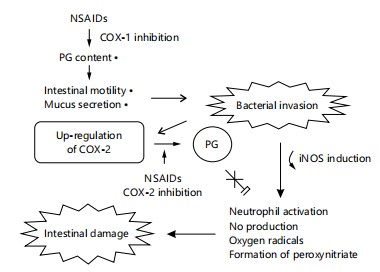
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): The NSAIDs are a major cause of peptic ulcers, especially in older adults. They inhibit cyclooxygenase (COX) enzymes, particularly COX-1, thereby reducing prostaglandin synthesis. Prostaglandins play a crucial role in maintaining gastric mucosal integrity by promoting mucus and bicarbonate secretion, maintaining mucosal blood flow, and facilitating epithelial repair. The NSAID use compromises these protective mechanisms, leading to increased vulnerability to gastric acid and pepsin. The NSAIDs may also cause direct topical irritation to the gastric lining27. The risk increases with high doses, prolonged use, concurrent use of corticosteroids or anticoagulants, and in individuals infected with H. pylori28 (Fig. 2).
Figure 2 shows that Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) can induce ulcers by disrupting the protective mechanisms of the gastrointestinal lining. Normally, prostaglandins help maintain mucosal defense by stimulating mucus and bicarbonate secretion, maintaining blood flow, and regulating acid production. The NSAIDs inhibit cyclooxygenase (COX) enzymes, which reduce prostaglandin synthesis. This impairs mucosal protection, making the stomach and duodenum more vulnerable to gastric acid. Additionally, NSAIDs have direct topical irritant effects on the mucosa, further increasing injury. The combined effects lead to erosion, ulcer formation, and potential complications such as bleeding, perforation, or obstruction.
Stress: Severe physiological stress, particularly from critical illness, trauma, burns (Curling’s ulcers), or major surgery, can precipitate stress-related mucosal damage and ulceration. Stress ulcers typically occur in the stomach and proximal duodenum1. The pathogenesis involves hypoperfusion of the gastric mucosa, leading to ischemia, impaired mucus-bicarbonate barrier, and increased acid back-diffusion2. Neuroendocrine responses to stress (e.g., catecholamine and cortisol surges) also impair mucosal defenses. While psychological stress alone is less likely to cause ulcers, it can exacerbate symptoms and delay healing by influencing behaviors (e.g., smoking, alcohol intake) and possibly altering gastric physiology3.
Lifestyle factors: Various lifestyle habits contribute to the development and exacerbation of peptic ulcers. Cigarette smoking impairs mucosal healing, reduces bicarbonate secretion, and increases gastric acid production. Chronic alcohol consumption damages the gastric mucosa directly and disrupts mucosal barrier function4. Dietary factors such as highly spicy or acidic foods are often implicated, though evidence of a direct causal link is limited; however, they may aggravate symptoms. Poor dietary habits and irregular meals can influence acid secretion patterns. Additionally, high caffeine intake may increase acid production. Together, these factors compromise mucosal defenses and synergize with other risk factors (e.g., H. pylori, NSAIDs) to promote ulcer formation5.
Non-operative management strategies of perforated peptic ulcer disease: Perforated Peptic Ulcer Disease (PPUD) remains a surgical emergency with significant morbidity and mortality, particularly in elderly patients or those with comorbidities6. Traditionally managed operatively, a non-operative or conservative approach has gained acceptance in selected patients based on clinical and radiological criteria. The goal is to manage the perforation without surgery while closely monitoring for deterioration. This comprehensive discussion explores the selection criteria for non-operative management and details the essential components of conservative treatment7.
Selection criteria for non-operative approach: Non-operative management (NOM) of PPUD is not suitable for all patients. Careful patient selection is critical to avoid missed treatment windows for necessary surgery. The ideal candidate for conservative treatment exhibits the following features:
| • | Hemodynamic stability: Patients must have stable vital signs (normal blood pressure and heart rate) without signs of shock or ongoing bleeding. Hemodynamic instability often suggests a more severe perforation or complication requiring surgical intervention8 | |
| • | Hemodynamic stability: Patients must have stable vital signs (normal blood pressure and heart rate) without signs of shock or ongoing bleeding. Hemodynamic instability often suggests a more severe perforation or complication requiring surgical intervention8 | |
| • | Absence of generalized peritonitis: Localized abdominal tenderness without signs of generalized peritonitis (rebound tenderness, guarding, and rigidity) suggests a contained perforation. Generalized peritonitis, in contrast, indicates widespread contamination and requires urgent surgery9 | |
| • | Radiological evidence of a sealed or localized perforation: Imaging studies, particularly abdominal CT scans, are crucial. Minimal free air, absence of free fluid, and presence of a sealed perforation (localized collection or omental patch) support non-operative management. A lack of extensive pneumoperitoneum or peritoneal fluid is essential10 | |
| • | Early presentation: Patients presenting within 24 hrs of symptom onset generally respond better to conservative treatment. Delayed presentation increases the risk of peritoneal contamination and sepsis, often necessitating surgery11 | |
| • | Absence of severe comorbidities: Patients should not have severe immunosuppression, uncontrolled diabetes, or chronic renal failure, as these conditions may compromise healing and mask signs of deterioration12 | |
| • | Close monitoring availability: Patients must be managed in a hospital setting with the capability for intensive monitoring and prompt surgical backup if conservative treatment fails13 | |
| • | Patient consent and compliance: The patient must understand the risks and benefits of conservative treatment and be compliant with bed rest, Nil Per Os, and continuous monitoring14 |
Components of conservative treatment: Once a patient is deemed suitable for non-operative management, the following components form the backbone of treatment. Each element targets stabilization, infection control, acid suppression, and ulcer healing15.
| • | Nil Per Os (NPO): The first and most basic step in non-operative management is keeping the patient nil per os. This prevents further gastric secretion and limits peritoneal contamination. Complete bowel rest allows the gastrointestinal tract to recover and supports natural sealing of the perforation. Nutritional support, if required, is provided parenterally until oral intake can be resumed, typically after 48-72 hrs of clinical improvement and imaging confirmation of perforation containment16 | |
| • | Nasogastric decompression: Insertion of a nasogastric (NG) tube serves multiple purposes in conservative management. By continuously aspirating gastric contents, the NG tube minimizes the risk of further leakage through the perforation and reduces gastric distension. Decompression helps relieve symptoms such as vomiting and reduces the risk of aspiration in debilitated patients. In many cases, the NG tube is kept in place until the patient has stabilized and shows signs of reduced inflammation, at which point it may be clamped and removed gradually17 | |
| • | Intravenous fluid resuscitation: Perforated ulcers can lead to significant fluid loss into the peritoneal cavity, causing hypovolemia and electrolyte imbalances. Prompt and aggressive intravenous fluid resuscitation is essential to restore circulating volume, correct electrolyte disturbances, and maintain adequate organ perfusion. Isotonic crystalloids such as normal saline or lactated Ringer’s solution are typically used. Fluid therapy is guided by vital signs, urine output, and serial laboratory measurements to ensure appropriate hydration without fluid overload18 | |
| • | Broad-spectrum antibiotics: Since perforation allows gastrointestinal flora to enter the peritoneal cavity, initiating empirical broad-spectrum antibiotic therapy is crucial to prevent or treat secondary peritonitis. Antibiotics should target both aerobic and anaerobic organisms commonly found in the gastrointestinal tract. A typical regimen includes a third-generation cephalosporin (e.g., ceftriaxone) combined with metronidazole. Alternatively, monotherapy with a beta-lactam/beta-lactamase inhibitor such as piperacillin-tazobactam may be used19. The duration of antibiotic therapy is generally 5-7 days, adjusted based on clinical response and microbiological results | |
| • | Proton Pump Inhibitors (PPIs): The PPIs are vital for reducing gastric acid secretion, promoting ulcer healing, and preventing further mucosal damage. High-dose intravenous PPIs (e.g., pantoprazole 40-80 mg IV twice daily) are typically initiated. By suppressing gastric acid, PPIs aid in creating a more favorable environment for ulcer closure and reduce the risk of reperforation. Once the patient shows improvement and tolerates oral intake, IV PPIs can be switched to oral formulations, continuing for at least 4-8 weeks20 | |
| • | Monitoring and supportive care: Close clinical monitoring is a cornerstone of non-operative management. Patients must be frequently assessed for signs of deterioration, including: | |
| • | Increasing abdominal pain or distension | |
| • | Rising white blood cell count or CRP | |
| • | Hemodynamic instability | |
| • | Persistent fever | |
| • | Ongoing sepsis or failure to respond to therapy |
Serial abdominal examinations, vital sign monitoring, urine output tracking, and repeated laboratory tests are performed regularly. In some cases, repeat imaging (CT abdomen) may be warranted to assess for signs of abscess formation or failure of the sealed perforation. Supportive care also includes pain management with parenteral analgesics (preferably non-NSAID medications), oxygen supplementation as needed, thromboprophylaxis, and consideration for nutritional support21. If no clinical or radiological improvement is noted within 24-48 hrs, surgical intervention is reconsidered to avoid complications like generalized peritonitis or sepsis.
Clinical outcomes of non-operative management of Perforated Peptic Ulcer Disease (PPUD): Non-operative management (NOM) of Perforated Peptic Ulcer Disease (PPUD) has emerged as a viable treatment approach in selected patients, particularly those who are hemodynamically stable, have minimal peritoneal contamination, and exhibit no signs of generalized sepsis. This conservative approach includes Nil Per Os (NPO), nasogastric decompression, intravenous Proton Pump Inhibitors (PPIs), antibiotics, and close clinical monitoring22. Non-operative management of PPUD offers a safe and effective alternative to surgical intervention in carefully selected patients. Clinical outcomes such as morbidity, mortality, hospital stay, and patient satisfaction are generally favorable when the criteria for conservative management are strictly followed. However, close monitoring is essential to detect complications early, particularly abscess formation, sepsis, or treatment failure necessitating delayed surgery. With careful patient selection, timely diagnosis, and a structured management protocol, NOM can be an optimal strategy that minimizes invasiveness while preserving patient quality of life23.
Below is a discussion of the clinical outcomes associated with NOM under the key headings.
Morbidity and mortality rates: The morbidity and mortality outcomes of non-operative management depend on several factors, including patient selection, timing of intervention, and co-morbid conditions. In well-selected cases, NOM has shown favorable morbidity and mortality rates comparable to surgical intervention.
| • | Morbidity: Studies have reported morbidity rates ranging from 10 to 35% in NOM of PPUD. Common morbidities include localized peritonitis, delayed abscess formation, and electrolyte imbalances. These complications are more frequently observed in elderly patients, those with comorbidities, or delayed presentation. However, when applied to younger, stable patients with early diagnosis, the incidence of complications is significantly reduced24 | |
| • | Mortality: Mortality rates for NOM are generally low in appropriate patient populations, often cited between 5 and 10%. In contrast, surgical management may carry a higher mortality, especially in elderly or high-risk patients. The main causes of mortality in NOM are sepsis and multi-organ failure secondary to unrecognized worsening perforation or complications. When conservative treatment fails and delayed surgery is required, the risk of death increases, especially if there is significant peritoneal contamination or septic shock. Overall, NOM can be associated with acceptable morbidity and mortality, especially when early diagnosis, proper imaging, and close monitoring are ensured25 |
Hospital stay duration: The duration of hospitalization is an important outcome in assessing the efficacy and cost-effectiveness of any medical management strategy. In NOM of PPUD, the average hospital stay is typically 7 to 10 days, depending on the patient's response to conservative therapy. This duration may be shorter than that associated with surgical treatment, which often involves post-operative recovery, wound care, and possible surgical complications26.
However, hospital stay in NOM may be prolonged if complications arise or if the patient’s response is slow, necessitating extended monitoring or further imaging. Factors influencing hospital stay duration include:
| • | Time to symptom resolution (e.g., cessation of abdominal pain and fever) | |
| • | Resumption of oral intake | |
| • | Control of infection or peritonitis | |
| • | Absence of need for surgical conversion |
Patients with uncomplicated PPUD managed non-operatively often recover more quickly, experience less post-treatment pain, and resume oral intake earlier than post-surgical counterparts, potentially leading to reduced hospital costs and length of stay27.
Complication rates: While non-operative management avoids surgical risks, it is not without complications. The most common complications include:
| • | Intra-abdominal abscess formation: This occurs in approximately 5-15% of NOM cases. These abscesses are usually localized and may develop due to incomplete containment of gastric contents following perforation. Ultrasound or CT-guided percutaneous drainage is often effective in such cases, though some may ultimately require surgical intervention28 | |
| • | Sepsis and peritonitis: If the perforation is not adequately sealed or if peritoneal contamination is underestimated, patients may develop Systemic Inflammatory Response Syndrome (SIRS) or sepsis. Close monitoring and early escalation to surgery are crucial in such cases. The risk of sepsis is higher in older patients or those with immunosuppression or delayed presentation1 | |
| • | Pneumoperitoneum and paralytic ileus: Persistent pneumoperitoneum is a radiological finding often seen in NOM, which may not always indicate treatment failure. However, its persistence beyond 5-7 days without clinical improvement may warrant reconsideration of the management plan2 | |
| • | Pulmonary complications: Atelectasis, aspiration pneumonia, or pleural effusions may occur in bedridden or elderly patients under NOM, particularly if nasogastric decompression is prolonged. Timely detection and management of these complications can significantly improve the outcomes of NOM and reduce long-term morbidity3 |
Re-perforation and need for delayed surgery: Re-perforation is one of the critical concerns in NOM. It typically occurs if the ulcer fails to seal spontaneously or if ulcerogenic factors such as NSAID use, H. pylori infection, or uncontrolled acid secretion persist.
| • | Re-perforation rates: They are relatively low in successful NOM, ranging between 5 and 10%. However, if NOM fails and re-perforation occurs, emergency surgery becomes inevitable, often under less favorable conditions than primary surgery4 | |
| • | Delayed surgery: Delayed surgery is required in about 10-20% of patients initially treated with conservative management. Indications include: Worsening abdominal pain, signs of peritonitis or sepsis, failure to improve clinically within 48-72 hrs, radiologic evidence of increasing pneumoperitoneum or fluid collections. Delayed surgery may carry higher risks due to increased inflammation, adhesions, and systemic compromise. Nevertheless, early identification of NOM failure and prompt surgical intervention helps mitigate these risks. Predictors of NOM failure include: Advanced age, high APACHE II score, elevated serum lactate, and generalized peritonitis on imaging5 |
Quality of life and patient satisfaction: Quality of Life (QoL) and patient satisfaction are important long-term outcomes in assessing the success of NOM for PPUD. While immediate medical outcomes like morbidity and mortality are important, long-term well-being and functional recovery are equally vital6.
| • | Patient-reported outcomes: This suggests that individuals treated non-operatively often have less post-treatment pain, faster return to normal activities, lower rates of post-treatment complications like wound infections or hernias, and less psychological distress associated with surgery. However, QoL may be negatively affected in patients who experience treatment failure or require delayed surgery due to prolonged hospitalization, uncertainty, or repeated interventions7 | |
| • | Patient satisfaction with NOM: This is generally high when treatment is successful and uncomplicated. Clear communication, reassurance, and involvement in decision-making further enhance satisfaction levels. Nevertheless, patients must be adequately informed of the potential for delayed surgery and complications, and provided with close follow-up care, including H. pylori eradication therapy (if applicable), long-term PPI use, lifestyle modification (cessation of NSAIDs, smoking, alcohol), and regular endoscopic surveillance when indicated8 |
Prognostic factors influencing outcomes of non-operative management of Perforated Peptic Ulcer Disease (PPUD):
| • | Age and comorbidities: Age is a critical determinant of outcomes in non-operative management (NOM) of PPUD. Elderly patients, particularly those over 70 years, tend to have poorer outcomes due to reduced physiological reserves, delayed symptom recognition, and increased susceptibility to sepsis. Additionally, age-related decline in immune function and organ reserve complicates recovery9. Comorbidities such as diabetes mellitus, cardiovascular disease, chronic kidney disease, and chronic obstructive pulmonary disease significantly increase the risk of complications, including septic shock and multiorgan failure. The Charlson Comorbidity Index is often used to quantify the burden of comorbidities, with higher scores correlating with increased mortality. Patients with multiple or poorly controlled comorbidities are less likely to respond favorably to conservative therapy and may require surgical intervention10 | |
| • | Size and location of perforation: The size and anatomical site of the perforation greatly influence prognosis. Small perforations (<5 mm) are more amenable to NOM, particularly if promptly diagnosed and contained. In contrast, large perforations (>10 mm) often lead to diffuse peritonitis and are less likely to seal spontaneously, necessitating surgical repair11. Regarding location, duodenal ulcers, which are typically anterior and proximal, tend to perforate more often than gastric ulcers. Duodenal perforations usually respond better to conservative therapy due to better vascular supply and less contamination, whereas posterior gastric or pyloric perforations may be associated with severe peritonitis and higher morbidity12 | |
| • | Time to treatment initiation: Time from symptom onset to initiation of NOM is a critical prognostic factor. Early diagnosis and initiation of treatment (within 6-12 hrs) significantly improve outcomes by limiting peritoneal contamination and systemic inflammatory response. Delays beyond 24 hrs are associated with increased risk of sepsis, abscess formation, and failure of conservative therapy. Prompt initiation of intravenous antibiotics, proton pump inhibitors, nasogastric decompression, and close monitoring is essential for favorable outcomes13 | |
| • | Radiological findings: Imaging plays a vital role in both diagnosis and prognosis. The presence of pneumoperitoneum on upright chest or abdominal X-rays or CT scans confirms perforation. However, extensive free air or signs of peritoneal fluid accumulation may indicate a large or ongoing leak, which negatively impacts outcomes. Localized air with minimal fluid suggests a sealed or contained perforation, which is more likely to respond to NOM. The CT imaging can also help assess abscess formation, which if present, might necessitate drainage or surgical intervention14 | |
| • | Laboratory parameters: Certain laboratory values are predictive of the severity of illness and outcome. Elevated White Blood Cell (WBC) counts and C-Reactive Protein (CRP) levels reflect systemic inflammation and possible sepsis. Leukocytosis (>12,000/μL) and markedly raised CRP (>100 mg/L) are associated with poor prognosis and increased likelihood of NOM failure. Hypoalbuminemia and elevated serum lactate are additional indicators of systemic compromise. Serial monitoring of these parameters is vital for early detection of clinical deterioration15 |
Based on the findings of this comprehensive review on the outcomes of non-operative management (NOM) of Perforated Peptic Ulcer Disease (PPUD), several recommendations can be made to optimize patient outcomes16. The NOM should be reserved for carefully selected patients with minimal symptoms, no signs of generalized peritonitis, stable hemodynamics, and imaging evidence of contained perforation, with early and accurate diagnosis through clinical assessment and imaging, particularly CT scanning, being crucial in guiding treatment decisions. Standardized protocols incorporating Nil Per Os (NPO), nasogastric decompression, intravenous Proton Pump Inhibitors (PPIs), broad-spectrum antibiotics, and close clinical monitoring should be adopted to enhance consistency and success rates17. Patients undergoing NOM must be managed in facilities with immediate access to surgical intervention in case of clinical deterioration, with regular assessment for signs of sepsis or worsening abdominal symptoms being vital. Furthermore, risk stratification tools should be developed and validated to aid in identifying appropriate candidates for conservative management18. Finally, more robust prospective studies and randomized controlled trials are required to strengthen the evidence base, define clear selection criteria, and determine long-term outcomes, including recurrence and quality of life. Implementing these recommendations can help reduce morbidity, improve resource utilization, and ensure safe, effective care for PPUD patients managed non-operatively19.
CONCLUSION
Non-operative management (NOM) of Perforated Peptic Ulcer Disease (PPUD) is a viable alternative to surgery in carefully selected patients. Evidence indicates that NOM is effective in hemodynamically stable patients without generalized peritonitis or sepsis, offering reduced morbidity, shorter hospital stays, and lower healthcare costs, particularly in elderly or high-risk populations. Radiological imaging, especially CT scans, is essential for diagnosis, monitoring, and guiding decisions. However, delayed surgical intervention in deteriorating patients substantially increases mortality, highlighting the importance of timely recognition of treatment failure. Although surgery remains the standard for complicated cases, NOM is a safe and effective option for selected patients when applied with strict clinical vigilance and multidisciplinary oversight. Further research should refine patient selection criteria, establish standardized protocols, and provide large-scale prospective evidence to better define its role.
SIGNIFICANCE STATEMENT
This review highlights the growing role of non-operative management (NOM) in the treatment of Perforated Peptic Ulcer Disease (PPUD). By synthesizing evidence across clinical studies, it demonstrates that NOM can be safe and effective in carefully selected, hemodynamically stable patients, particularly the elderly or those at high surgical risk. The findings emphasize the importance of imaging, strict clinical monitoring, and timely recognition of treatment failure. This work contributes to refining patient selection criteria, underscores the need for standardized protocols, and identifies areas where further large-scale trials are required. Ultimately, it supports a more individualized, evidence-based approach to PPUD management that may reduce morbidity, hospitalization time, and healthcare costs without compromising patient safety.
ACKNOWLEDGMENT
We sincerely acknowledge all authors for their contributions that make this work a success.
REFERENCES
- Agrez, M.V., D.A. Henry, S. Senthiselvan and J.M. Duggan, 1992. Changing trends in perforated peptic ulcer during the past 45 years. Aust. N.Z. J. Surg., 62: 729-732.
- Ali, A.M., A.N. Mohamed, Y.G. Mohamed and S.İ. Keleşoğlu, 2022. Clinical presentation and surgical management of perforated peptic ulcer in a tertiary hospital in Mogadishu, Somalia: A 5-year retrospective study. World J. Emerg. Surg., 17.
- Vázquez, J.A.A., K. Khodakaram, M. Bergström and P.O. Park, 2021. Stent treatment or surgical closure for perforated duodenal ulcers: A prospective randomized study. Surg. Endoscopy, 35: 7183-7190.
- Boey J., S.K.Y. Choi, T.T. Alagaratnam and A. Poon, 1987. Risk stratification in perforated duodenal ulcers: A prospective validation of predictive factors. Ann. Surg., 205: 22-32.
- Chung, K.T. and V.G. Shelat, 2017. Perforated peptic ulcer-an update. World J. Gastrointestinal Surg., 9: 1-12.
- Crofts, T.J., K.G.M. Park, R.J.C. Steele, S.S.C. Chung and A.K.C. Li, 1989. A randomized trial of nonoperative treatment for perforated peptic ulcer. N. Engl. J. Med., 320: 970-973.
- Das, R., S. Sureshkumar, G.S. Sreenath and V. Kate, 2016. Sequential versus concomitant therapy for eradication of Helicobacter pylori in patients with perforated duodenal ulcer: A randomized trial. Saudi J. Gastroenterol., 22: 309-315.
- Slaathaug, C., M.M. Paulsen, S. Jafarzadeh, M.H. Carlsen and L.F. Andersen, 2024. Nutritional quality and climate impact of Norwegian adults’ diet classified according to the NOVA system. Nutr. J., 23.
- Donovan, A.J., T.V. Berne and J.A. Donovan, 1998. Perforated duodenal ulcer: An alternative therapeutic plan. Arch. Surg., 133: 1166-1171.
- Gatta, L., N. Vakil, D. Vaira and C. Scarpignato, 2013. Global eradication rates for Helicobacter pylori infection: Systematic review and meta-analysis of sequential therapy. BMJ, 347.
- Gisbert, J.P., S. Khorrami, F. Carballo, X. Calvet, E. Gene and E. Dominguez-Muñoz, 2004. Helicobacter pylori eradication therapy vs. antisecretory non-eradication therapy for the prevention of recurrent bleeding from peptic ulcer. Aliment. Pharmacol. Ther., 19: 617-629.
- Gupta, S., A.A. Alawad, K. Dacosta, A. Mahmoud and T. Mohammed, 2022. Operative versus non-operative management for perforated peptic ulcer disease. Ann. Med. Surg., 82.
- Umaru, I.J., A.S. Osagie, A.M. Chizoba and M.A. Adondua, 2023. Antiulcer effects of the methanolic root extracts of Paulownia elongata on indomethacin-induced peptic ulcer in male albino rats. World J. Adv. Res. Rev., 19: 178-188.
- Ishiguro, T., Y. Kumagai, H. Baba, Y. Tajima and H. Imaizumi et al., 2014. Predicting the amount of intraperitoneal fluid accumulation by computed tomography and its clinical use in patients with perforated peptic ulcer. Int. Surg., 99: 824-829.
- Karabulut, K., M. Dinçer, R.K. Liman and S. Usta, 2019. Non-operative management of perforated peptic ulcer: A single center experience. Turk. J. Trauma Emerg. Surg., 25: 585-588.
- Khan, O.A., J. Dunning, A.C. Parvaiz, R. Agha, D. Rosin and K. Mackway-Jones, 2011. Towards evidence-based medicine in surgical practice: Best BETs. Int. J. Surg., 9: 585-588.
- Knaus, W.A., E.A. Draper, D.P. Wagner and J.E. Zimmerman, 1985. APACHE II: A severity of disease classification system. Crit. Care Med., 13: 818-829.
- Malfertheiner, P., F. Megraud, C.A. O'Morain, J. Atherton and A.T.R. Axon et al., 2012. Management of Helicobacter pylori infection-The maastricht IV/florence consensus report. Gut, 61: 646-664.
- Noguiera, C., A.S. Silva, J.N. Santos, A.G. Silva, J. Ferreira, E. Matos and H. Vilaça, 2003. Perforated peptic ulcer: Main factors of morbidity and mortality. World J. Surg., 27: 782-787.
- Mizanur Rahuman, M., A.K. Saha and Abdur Rahim, 2011. Experience of peptic ulcer perforation over a decade in a teaching hospital of Southern Bangladesh. Ceylon Med. J., 48: 53-55.
- Satoh, K., J. Yoshino, T. Akamatsu, T. Itoh and M. Kato et al., 2016. Evidence-based clinical practice guidelines for peptic ulcer disease 2015. J. Gastroenterol., 51: 177-194.
- Surapaneni, S., S. Rajkumar and A.V.B. Reddy, 2013. The perforation-operation time Interval; an Important mortality indicator in peptic ulcer perforation. J. Clin. Diagn. Res., 7: 880-882.
- Svanes, C., H. Salvesen, L. Stangeland, K. Svanes and O. Soreide, 1993. Perforated peptic ulcer over 56 years. Time trends in patients and disease characteristics. Gut, 34: 1666-1671.
- Tarasconi, A., F. Coccolini, W.L. Biffl, M. Tomasoni and L. Ansaloni et al., 2020. Perforated and bleeding peptic ulcer: WSES guidelines. World J. Emerg. Surg., 15.
- Thomsen, R.W., A. Riis, S. Christensen, M. Norgaard and H.T. Sorensen, 2006. Diabetes and 30-day mortality from peptic ulcer bleeding and perforation: A Danish population-based cohort study. Diabetes Care, 29: 805-810.
- Yoon, H., D.H. Lee, E.S. Jang, J. Kim and C.M. Shin et al., 2015. Optimal initiation of Helicobacter pylori eradication in patients with peptic ulcer bleeding. World J. Gastroenterol., 21: 2497-2503.
- Zagari, R.M., M. Romano, V. Ojetti, R. Stockbrugger and S. Gullini et al., 2015. Guidelines for the management of Helicobacter pylori infection in Italy: The III Working Group Consensus Report 2015. Digestive Liver Dis., 47: 903-912.
- Zelickson, M.S., C.M. Bronder, B.L. Johnson, J.A. Camunas and D.E. Smith et al., 2011. Helicobacter pylori is not the predominant etiology for peptic ulcers requiring operation. Am. SurgeonTM, 77: 1054-1060.
How to Cite this paper?
APA-7 Style
Abah,
M.A., Ikedionwu,
O.I., Oluwatoyin,
O.I., Oputa,
P.U., Victor,
J.A., Chikelum,
E.P. (2025). Non-Operative Management of Perforated Peptic Ulcer Disease: Outcomes and Evidence Review. Trends in Medical Research, 20(1), 64-75. https://doi.org/10.3923/tmr.2025.64.75
ACS Style
Abah,
M.A.; Ikedionwu,
O.I.; Oluwatoyin,
O.I.; Oputa,
P.U.; Victor,
J.A.; Chikelum,
E.P. Non-Operative Management of Perforated Peptic Ulcer Disease: Outcomes and Evidence Review. Trends Med. Res 2025, 20, 64-75. https://doi.org/10.3923/tmr.2025.64.75
AMA Style
Abah
MA, Ikedionwu
OI, Oluwatoyin
OI, Oputa
PU, Victor
JA, Chikelum
EP. Non-Operative Management of Perforated Peptic Ulcer Disease: Outcomes and Evidence Review. Trends in Medical Research. 2025; 20(1): 64-75. https://doi.org/10.3923/tmr.2025.64.75
Chicago/Turabian Style
Abah, Moses, Adondua, Onyinye Ifeoma Ikedionwu, Obagade Ibukunoluwa Oluwatoyin, Praise Udoka Oputa, Jemiseye Abayomi Victor, and Ezeudu Paschal Chikelum.
2025. "Non-Operative Management of Perforated Peptic Ulcer Disease: Outcomes and Evidence Review" Trends in Medical Research 20, no. 1: 64-75. https://doi.org/10.3923/tmr.2025.64.75

This work is licensed under a Creative Commons Attribution 4.0 International License.