Effect of Toll-Like Receptor 4 on Angiotensin II-Induced Cardiac Hypertrophy in Mice
-
Junjun Shang
Panzhihua Key Laboratory of Cardiomyopathy and Heart Failure, Affiliated Hospital of Panzhihua University, Panzhihua, Sichuan 617099, China
Hailong LinAffiliated Dalian Central Hospital, Dalian Medical University, Dalian, Liaoning 116000, China
Yuqing TianAffiliated Dalian Central Hospital, Dalian Medical University, Dalian, Liaoning 116000, China
Lin Wu
Panzhihua Key Laboratory of Cardiomyopathy and Heart Failure, Affiliated Hospital of Panzhihua University, Panzhihua, Sichuan 617099, China
| Received 25 Sep, 2023 |
Accepted 02 Nov, 2023 |
Published 05 Nov, 2023 |
Background and Objective: The TLR4 plays an important role in the development of cardiovascular disease and is closely related to cardiac inflammation. This study aimed to investigate the role of TLR4 in Ang II-induced cardiac hypertrophy. Materials and Methods: The Ang II-induced cardiac hypertrophy model in C57BL/6 male mice was established and treated with TAK-242 for 4 weeks. The cross-sectional area of cardiomyocytes was evaluated by Hematoxylin and Eosin (H&E) staining. Cardiac fibrosis was measured with Masson staining. Vimentin expression was detected by immunohistochemistry. The mRNA expression of TLR4 was analyzed by RT-qPCR. Results: The Ang II-increased cardiac mass index, cardiac-tibial ratio, cross-sectional area of cardiomyocytes and cardiac fibrosis as well as vimentin and TLR4 expression. Administration of TAK-242 attenuated these effects induced by Ang II. Conclusion: The TLR4 plays a vital role in Ang II-induced cardiac hypertrophy. It provides a new target for the future treatment of cardiac hypertrophy.
| Copyright © 2023 Shang et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Myocardial hypertrophy is a common morphological change in cardiovascular disease1. Although the early physiological myocardial hypertrophy is the adaptive compensation of the heart to the hemodynamic load and can temporarily maintain the need for blood supply to the body, with the extension of time. The structure and function of cardiomyocytes have changed significantly, from physiological myocardial hypertrophy to pathological myocardial hypertrophy, resulting in heart failure and even sudden cardiac death2.
As a pattern recognition receptor, Toll-Like Receptors (TLRs) are widely expressed in many human tissues. It can participate in the pathological process of cardiovascular diseases such as coronary heart disease and heart failure, inflammatory diseases such as severe septicemia and chronic infection, tumors and other diseases by recognizing corresponding ligands, among which TLR4 plays a particularly significant role3,4. Toll-Like Receptor 4 (TLR4) mediates cardiac inflammation, which plays an important role in the development of cardiovascular disease and the increase of its level is a strong risk factor for cardiovascular disease5,6. Liu et al.7 found that in congestive heart failure caused by myocardial infarction, inflammatory cytokines are increased in serum and heart and the expression of TLR4 is increased. Injection of lentivirus shRNA targeting TLR4 into the infarcted heart can reduce the production of inflammatory cytokines, reduce the infarct size and improve cardiac function. Dange et al.8 reported that in the hypertensive model, male SD rats treated with the TLR4 inhibitor showed a significant decrease in myocardial inflammation and iNOS expression, indicating that TLR4 blockade inhibited the hypertensive response, resulting in a down-regulation of myocardial inflammatory activity.
The TAK-242 is a specific inhibitor of TLR4, which can block the transmission of TLR4 signal to the cell and weaken the inflammatory response9. Studies show that TAK-242 can prevent tissue damage mediated by inflammatory response10. Wang et al.11 and Su et al.12 found that TAK-242 significantly inhibited TLR4/MyD88/NF-κB signal transduction, decreased the expression of TLR4 in the myocardium, decreased the expression of inflammatory cytokines such as TNF-α, IL-1β and IL-18, reduced the activation of NLRP3 inflammasome and improved cardiac function. The aim of this experiment was to study the role of TLR4 in Angiotensin II (Ang II)-induced cardiac hypertrophy by applying TAK-242, which provided new ideas for inhibiting cardiac hypertrophy in clinical practice.
MATERIALS AND METHODS
Reagents and solutions: This study was conducted from 1st May, 2017 to 1st May, 2018, in the Dalian Central Hospital Central Laboratory of Dalian Medical University. Experimental animals (C57BL/6) were purchased from the Institute of Genetic Engineering Model Animals for Major Diseases of Dalian Medical University. The H&E staining kit (G1076), Masson staining kit (G1006), Immunohistochemical kit (G1215) and DAB chromogenic kit (G1212-200T) were purchased from Servicebio Biological Technology Co., Ltd. (Wuhan, China). The TAK-242 (614316) and Ang II (05-23-0101) was purchased from Sigma (Saint Louis, Missouri, USA). ALZET osmotic pumps (Model 2004) were purchased from DURECT Corporation (Cupertino, CA, USA). Anti-Vimentin Antibody (10366-1-AP) was purchased from Protein Tech (Wuhan, China). The Reverse Transcription kit was purchased from Thermo Fisher Scientific (Shanghai, China). The SYBR GREEN PCR master mix was bought from Roche (Basel, Switzerland).
Animal experiments: Twenty-one SPF C57BL/6 male mice, aged 8-10 weeks and weighing 20-25 g, were randomly divided into three groups: Control group (n = 7), Ang II group (n = 7) and Ang II+TAK-242 group (n = 7). The animal study was reviewed and approved by the animal ethics Committee of the Affiliated Dalian Central Hospital of Dalian Medical University. Osmotic pumps were implanted subcutaneously in all three groups. Normal saline was pumped continuously at the speed of 1.3 mg/kg/day in the control group. Ang II was pumped continuously at the speed of 1.3 mg/kg/day in Ang II and Ang II+TAK-242 groups13. The TAK-242 was injected intraperitoneal twice a week in Ang II+TAK-242 group.
Determination of whole heart mass index and cardio-tibial ratio: After 4 weeks of treatment, the mice were weighed and then killed by cervical dislocation. The heart was removed and weighed. The tibia was measured. The heart mass index = heart mass/body mass. The unit was mg g–1. The cardiac-tibial ratio = heart mass/tibia length. The unit was mg mm–1.
H&E staining: As 5 μm thick sections were prepared by gradient ethanol dehydration and routine paraffin embedding. After removing paraffin with xylene, the sections were stained with hematoxylin for about 3 min, differentiated with 1% dihydrochloride. The sections were then placed in eosin dye solution for 15-30 sec. The sections were dried and sealed with xylene clear and neutral resin. The morphology of the myocardial tissue was observed by light microscope (IX51, Olympus, Tokyo, Japan). Ten visual fields were randomly selected and 10 cells were selected from each visual field. The cross-sectional area of cardiomyocytes was measured using Image J software (1.49 version, NIH, Bethesda, Maryland, USA).
Masson staining: Thick sections of 5 μm were cut and stained. Paraffin sections were dewaxed with xylene and descending gradient alcohol, then treated with potassium dichromate mordant for 12-18 hrs and differentiated with 1% hydrogen chloride (HCl) alcohol until weak ammonia returned to blue. The slides were stained with ponceau acid fuchsin staining solution for 10 min and then treated with phosphorolybdic acid solution for 2 min. The slides were directly stained with aniline blue for 7 min, dried and sealed with xylene clear and neutral resin. Staining of collagen fibers was observed by light microscopy and five fields were randomly selected at high magnification. The staining results were quantified using image J. Masson staining analysis usually calculates the collagen volume fraction, namely the percentage of the collagen-positive blue area in the total tissue area.
Immunohistochemistry: The sections were cut at 3 μm and stained for immunohistochemistry. After dewaxing the paraffin sections, the paraffin sections were rehydrated in an antigen restoration instrument for approximately 2 hrs. After the anti-vimentin antibody was dropped on the slides, they were incubated at room temperature for 1 hr and the second antibody was dropped and then incubated at room temperature for 1 hr. Then the DAB (3,3 -Diaminobenzidine) chromogenic solution was added for 3-5 min. The nuclei were re-stained with hematoxylin, 1% hydrochloric acid alcohol and weak ammonia water, respectively. The slides were dried and sealed with xylene transparent and neutral resin. Vimentin staining was observed under a light microscope, five visual fields were randomly selected by high-power microscope and the staining results were quantitatively analyzed using Image J.
RT-qPCR: Thirty milligrams of mouse heart tissue were collected. Total RNA was extracted with Trizol lysate and reverse transcribed using the Reverse Transcription kit. The PCR experiment was performed according to the manual of the SYBR GREEN PCR master mix kit. The PCR reaction conditions were as follows: 95°C, 10 min, cycle 40 times at 95°C, 15 sec, 60°C, 60 sec. Using (Glyceraldehyde-3-phosphate dehydrogenase) as the reference gene, the PCR data were analyzed according to the 2-ΔΔCT method. The nucleotide sequences of TLR4 and GAPDH primers were as follows: TLR4 forward, GTGAGTAACCTTCTCCATGAGAGA and reverse, GCACTCTTAGCAAACCTCAGG; GAPDH forward, AGGTGGTGAAGCCGGCATCT and reverse, GGCATCGAAGGTGGAAGAGT.
Statistical analysis: GraphPad Prism 8.0 was used to analyze the data. Measurement data which followed a normal distribution were expressed as Mean±SEM. Comparison between groups was analyzed by t-test. The p<0.05 means the difference is statistically significant.
RESULTS
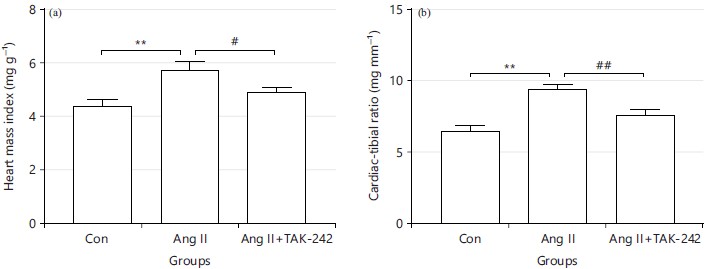
TAK-242 attenuates the increases of the cardiac mass index and cardiac-tibial ratio induced by Ang II: Compared with the control group, the heart mass index of the Ang II group was significantly higher (5.710±0.332 vs 4.386±0.222, **p<0.01, Fig. 1a). The heart mass index of the Ang II+TAK-242 group was lower than that of the Ang II group (4.900±0.157 vs 5.710±0.332, #p<0.05, Fig. 1a). The cardiac-tibial ratio in the Ang II group was obviously higher than that in the control group (9.327±0.408 vs 6.456±0.352, **p<0.01, Fig. 1a). After TAK-242 treatment, the cardiac-tibial ratio decreased (7.559±0.369 vs 9.327±0.408, #p<0.01, Fig. 1b).
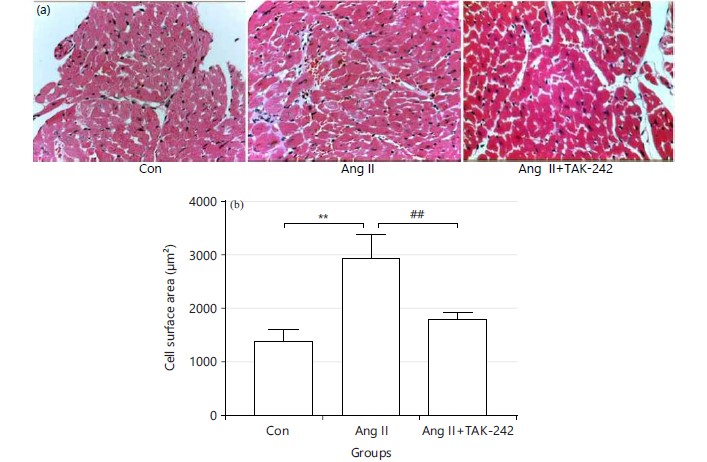
TAK-242 reduces cardiomyocyte cross-sectional area increased by Ang II: The HE staining showed that the cross-sectional area of cardiomyocytes in the Ang II group was larger than that in the control group (2926.089±417.838 vs 1387.924±202.383 μm2, **p<0.01, Fig. 2a-b). Compared with the Ang II group, the cross-sectional area of cardiomyocytes was reduced in the Ang II+TAK-242 group (1785.695±125.688 vs 2926.089±417.838 μm2, #p<0.01, Fig. 2a-b).
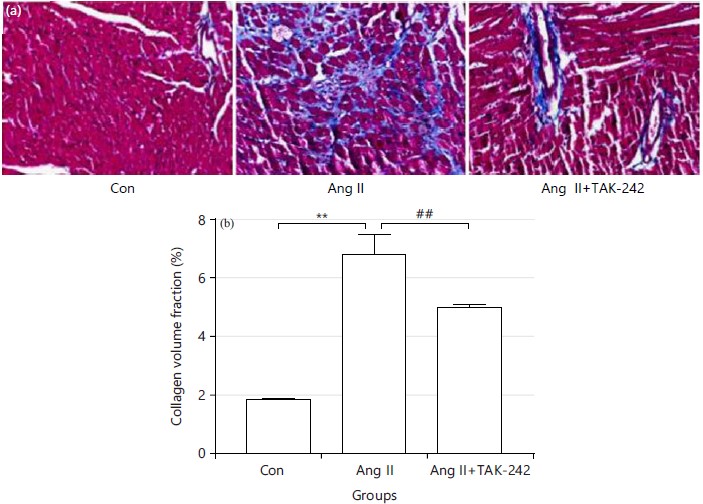
TAK-242 inhibits myocardial fibrosis induced by Ang II: Masson staining indicated that the collagen volume fraction in the Ang II group was significantly higher than that in the control group (6.810±0.656 vs 1.890±0.031, **p<0.01, Fig. 3a-b). The collagen volume fraction in the Ang II+TAK-242 group was less than that in the Ang II group (5.01±0.097 vs 6.810±0.656, #p<0.01, Fig. 3a-b).
|
|
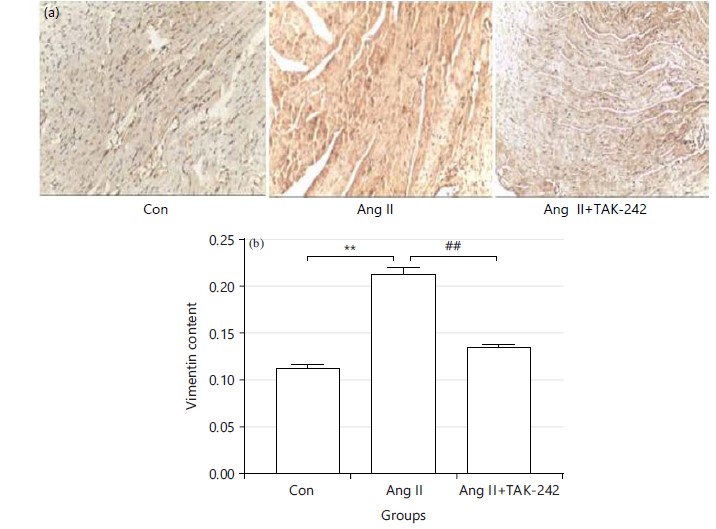
TAK-242 inhibits the increase of vimentin expression induced by Ang II: After immune histochemical staining, the expression of vimentin in the Ang II group was significantly higher than that in the control group (0.213±0.007 vs 0.112±0.004, **p<0.01, Fig. 4a-b). The expression of vimentin in the Ang II+TAK-242 group was lower than that in the Ang II group (0.136±0.002 vs 0.213±0.007, #p<0.01, Fig. 4a-b).
|
|
|
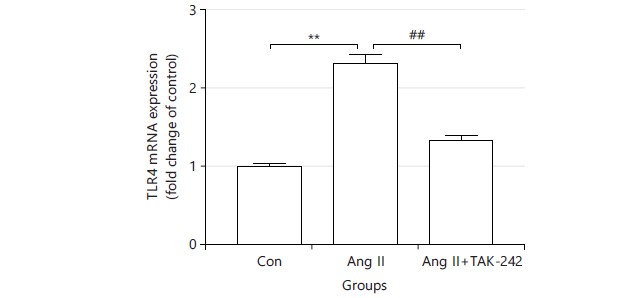
TAK-242 inhibits the increase of TLR4 expression induced by Ang II: Compared to the control group, the expression of TLR4 was significantly increased in the Ang II group (2.310±0.096 vs 1.000±0.028, **p<0.01, Fig. 5) and the expression of TLR4 was decreased after TAK-242 application (1.330±0.042 vs 2.310±0.096, #p<0.01, Fig. 5).
DISCUSSION
The Ang II caused the increases of whole heart mass index, cardiac-tibial ratio, cross-sectional area of cardiomyocytes, collagen fiber content, vimentin and TLR4 expression. The TAK-242, an inhibitor of TLR4, reduced these effects induced by Ang II. It suggests that TAK-242 may ameliorate cardiac hypertrophy induced by Ang II. The TLR4-mediated inflammation is involved in the regulation of myocardial remodeling during hypertrophy14. The TLR4 may act through MyD88 -dependent and TRIF-dependent pathways15.
The Ang II can induce the overexpression of Transforming Growth Factor-1 (TGF-1) in both autocrine and paracrine manner, induce the proliferation of cardiomyocytes and cardiac fibroblasts, promote the deposition of extracellular matrix proteins such as collagen and promote ventricular remodeling and hypertrophy16. The Ang II can induce cardiac hypertrophy through the oxidative stress pathway, an inflammatory response stimulated by increased Nuclear Transcription Factor κB (NFκB) activity and inhibition of the Mitogen-Activated Protein Kinase Pathway (MAPK)17-19. The Ang II has been shown to increase blood pressure and produce positive isotropic effects in addition to inducing myocardial growth (adaptive cardiac hypertrophy) and promoting angiogenesis, but long-term exposure to Ang II can lead to pathological cardiac hypertrophy and heart failure20. Vimentin is a component of fibroblasts and has been widely used to identify fibroblasts in vitro and in vivo21,22. Activation of fibroblasts is related to the severity of fibrosis. Cardiac fibroblasts are present in large numbers in the myocardium and are primarily involved in the myocardial fibrotic response, where they differentiate into synthetic and contractile myofibroblasts to maintain the structural integrity of the myocardium in response to injury such as inflammation or aging23,24. In this study, Ang II induced an increase in collagen fibers and vimentin content in the myocardium of mice and the TLR4 inhibitor was able to alleviate these effects. It suggests that TAK-242 can ameliorate Ang II-induced cardiac fibrosis and vimentin expression.
The TLRs are members of the pattern-recognition receptors (PRRs) family25. There are thirteen TLRs in mammals, which are expressed in almost all cells of the cardiovascular system. The TLR4 is mainly distributed in the cytoplasm of cardiomyocytes. The TLR4-mediated cytokines are involved in the
pathogenesis of cardiovascular disease26,27. Short-term activation of TLR4 has a protective effect on the cardiovascular system, but long-term or over-activation can induce the production of a variety of cytokines in the tissue, leading to myocardial remodeling28. Li et al.29 found that the expression of TLR4 is significantly increased in patients with hypertension, myocardial hypertrophy and heart failure. Activation of the TLR4/NF-κB signal is involved in the pathological process of hypertension, myocardial hypertrophy and heart failure. Inhibition of this signal may be one of the mechanisms by which telmisartan exerts its pharmacological effects. Jiang and Qu30 found that under the stimulation of LPS, the expression of TLR4 increased and myocardial remodeling occurred, while Ginkgo biloba Extract (GBE50) could inhibit myocardial remodeling by inhibiting the TLR4/NF-κB signal transduction system. Eißler et al.31 found that the expression of TLR4 and heart to body mass ratio increased with blood pressure elevation in hypertensive rats, suggesting that increased TLR4 expression and activity promotes global myocardial hypertrophy in established and progressive hypertension. This study showed that the cross-sectional area, fibrosis, vimentin expression and TLR4 expression of cardiomyocytes were increased by Ang II. While, TAK-242 decreased these effects. It suggests that inhibition of TLR4 may inhibit myocardial hypertrophy.
This study provides a reference for the clinical treatment of cardiac hypertrophy, but the depth of the study is insufficient. Measurement of MYD88 and related indices of downstream inflammatory factors such as IL-1β and TNF-α may be considered in future studies to further explore the molecular mechanism of the TLR4 inhibitor in the treatment of cardiac hypertrophy.
CONCLUSION
In a word, the application of TAK-242 reduced heart mass index and cardiac-tibial ratio, decreased cardiomyocyte cross-sectional area, ameliorated fibrosis, inhibited vimentin and TLR4 expression and ameliorated Ang II-induced cardiac hypertrophy. This research confirms that TLR4 is involved in cardiac hypertrophy and its inhibitor can reduce myocardial hypertrophy and provides a new breakthrough for clinical inhibition of myocardial hypertrophy.
SIGNIFICANCE STATEMENT
This experiment was mainly based on TAK-242 to investigate the role of TLR4 in Ang II-induced cardiac hypertrophy and to provide new ideas for clinical treatment of cardiac hypertrophy. This suggests that TLR4 is a key target in cardiac hypertrophy. It may help researchers to further investigate the role of other TLRs in Ang II-induced cardiac hypertrophy. This study provides a reference for the development of drugs related to inhibiting cardiac hypertrophy and the search for alternative drugs.
ACKNOWLEDGMENTS
This research was funded by Medical Science and Technology Project of Sichuan Provincial Health Commission, grant number 21PJ200; Provincial-level science and Technology Program Transfer Payment Special Fund project of Panzhihua Science and Technology Bureau, grant number 222ZYZF-S-01.
REFERENCES
- Hunter, J.J. and K.R. Chien, 1999. Signaling pathways for cardiac hypertrophy and failure. N. Engl. J. Med., 341: 1276-1283.
- Tham, Y.K., B.C. Bernardo, J.Y.Y. Ooi, K.L. Weeks and J.R. McMullen, 2015. Pathophysiology of cardiac hypertrophy and heart failure: Signaling pathways and novel therapeutic targets. Arch. Toxicol., 89: 1401-1438.
- Mann, D.L. and L. Kirschenbaum, 2011. The emerging role of innate immunity in the heart and vascular system. Circ. Res., 108: 1133-1145.
- Bhattacharyya, S., K. Kelley, D.S. Melichian, Z. Tamaki and F. Fang et al., 2013. Toll-like receptor 4 signaling augments transforming growth factor-β responses. Am. J. Pathol., 182: 192-205.
- Liu, M., J. Xie and Y. Sun, 2020. TLR4/MyD88/NF-κB-mediated inflammation contributes to cardiac dysfunction in rats of PTSD. Cell. Mol. Neurobiol., 40: 1029-1035.
- Yang, Y., J. Lv, S. Jiang, Z. Ma and D. Wang et al., 2016. The emerging role of toll-like receptor 4 in myocardial inflammation. Cell Death Dis., 7.
- Liu, L., Y. Wang, Z.Y. Cao, M.M. Wang and X.M. Liu et al., 2015. Up-regulated TLR4 in cardiomyocytes exacerbates heart failure after long-term myocardial infarction. J. Cell. Mol. Med., 19: 2728-2740.
- Dange, R.B., D. Agarwal, G.S. Masson, J. Vila, B. Wilson, A. Nair and J. Francis, 2014. Central blockade of TLR4 improves cardiac function and attenuates myocardial inflammation in angiotensin II-induced hypertension. Cardiovasc. Res., 103: 17-27.
- Kawamoto, T., M. Ii, T. Kitazaki, Y. Iizawa and H. Kimura, 2008. TAK-242 selectively suppresses Toll-like receptor 4-signaling mediated by the intracellular domain. Eur. J. Pharmacol., 584: 40-48.
- Zhang, Y., W. Peng, X. Ao, H. Dai, L. Yuan, X. Huang and Q. Zhou, 2015. TAK-242, a toll-like receptor 4 antagonist, protects against aldosterone-induced cardiac and renal injury. PLoS ONE, 10.
- Wang, X.T., Y.X. Lu, Y.H. Sun, W.K. He, J.B. Liang and L. Li, 2017. TAK-242 protects against apoptosis in coronary microembolization-induced myocardial injury in rats by suppressing TLR4/NF-κB signaling pathway. Cell. Physiol. Biochem., 41: 1675-1683.
- Su, Q., L. Li, Y. Sun, H. Yang, Z. Ye and J. Zhao, 2018. Effects of the TLR4/Myd88/NF-κB signaling pathway on NLRP3 inflammasome in coronary microembolization-induced myocardial injury. Cell. Physiol. Biochem., 47: 1497-1508.
- Zhang, L.N., V. da Cunha, B. Martin-McNulty, J. Rutledge, R. Vergona, M.E. Sullivan and Y.X. Wang, 2007. Monocyte chemoattractant protein-1 or macrophage inflammatory protein-1α deficiency does not affect angiotensin II-induced intimal hyperplasia in carotid artery ligation model. Cardiovasc. Pathol., 16: 231-236.
- Xiao, Z., B. Kong, H. Yang, C. Dai, J. Fang, T. Qin and H. Huang, 2020. Key player in cardiac hypertrophy, emphasizing the role of toll-like receptor 4. Front. Cardiovasc. Med., 7.
- Obayed Ullah, M., M.J. Sweet, A. Mansell, S. Kellie and B. Kobe, 2016. TRIF-dependent TLR signaling, its functions in host defense and inflammation, and its potential as a therapeutic target. J. Leukocyte Biol., 100: 27-45.
- Rosenkranz, S., M. Flesch, K. Amann, C. Haeuseler and H. Kilter et al., 2002. Alterations of β-adrenergic signaling and cardiac hypertrophy in transgenic mice overexpressing TGF-β1. Am. J. Physiol. Heart Circ. Physiol., 283: H1253-H1262.
- Kurdi, M. and G.W. Booz, 2011. New take on the role of angiotensin II in cardiac hypertrophy and fibrosis. Hypertension, 57: 1034-1038.
- Niu, J., Z. Jin, H. Kim and P.E. Kolattukudy, 2015. MCP-1-induced protein attenuates post-infarct cardiac remodeling and dysfunction through mitigating NF-κB activation and suppressing inflammation-associated microRNA expression. Basic Res. Cardiol., 110.
- Cardinale, J.P., S. Sriramula, N. Mariappan, D. Agarwal and J. Francis, 2012. Angiotensin II-induced hypertension is modulated by nuclear factor-κB in the paraventricular nucleus. Hypertension, 59: 113-121.
- Bhullar, S.K. and N.S. Dhalla, 2022. Angiotensin II-induced signal transduction mechanisms for cardiac hypertrophy. Cells, 11.
- Travers, J.G., F.A. Kamal, J. Robbins, K.E. Yutzey and B.C. Blaxall, 2016. Cardiac fibrosis: The fibroblast awakens. Circ. Res., 118: 1021-1040.
- Umbarkar, P., S. Ejantkar, S. Tousif and H. Lal, 2021. Mechanisms of fibroblast activation and myocardial fibrosis: Lessons learned from FB-specific conditional mouse models. Cells, 10.
- Gibb, A.A., M.P. Lazaropoulos and J.W. Elrod, 2020. Myofibroblasts and fibrosis: Mitochondrial and metabolic control of cellular differentiation. Circ. Res., 127: 427-447.
- Ivey, M.J. and M.D. Tallquist, 2016. Defining the cardiac fibroblast. Circ. J., 80: 2269-2276.
- Majewska, M. and M. Szczepanik, 2006. The role of toll-like receptors (TLR) in innate and adaptive immune responses and their function in immune response regulation. Adv. Hyg. Exp. Med., 60: 52-63.
- Jezierska, A., I.A. Kolosova and A.D. Verin, 2011. Toll like receptors signaling pathways as a target for therapeutic interventions. Curr. Signal Transduction Ther., 6: 428-440.
- O'Neill, L.A.J., C.E. Bryant and S.L. Doyle, 2009. Therapeutic targeting of toll-like receptors for infectious and inflammatory diseases and cancer. Pharmacol. Rev., 61: 177-197.
- Goulopoulou, S., C.G. McCarthy and R.C. Webb, 2016. Toll-like receptors in the vascular system: Sensing the dangers within. Pharmacol. Rev., 68: 142-167.
- Li, H.B., X. Li, C.J. Huo, Q. Su and J. Guo et al., 2016. TLR4/MyD88/NF-κB signaling and PPAR-γ within the paraventricular nucleus are involved in the effects of telmisartan in hypertension. Toxicol. Appl. Pharmacol., 305: 93-102.
- Jiang, H. and P. Qu, 2017. Effects of Ginkgo biloba leaf extract on local renin-angiotensin system through TLR4/NF-κB pathway in cardiac myocyte. Exp. Ther. Med., 14: 5857-5862.
- Eißler, R., C. Schmaderer, K. Rusai, L. Kühne and D. Sollinger et al., 2011. Hypertension augments cardiac Toll-like receptor 4 expression and activity. Hypertens. Res., 34: 551-558.
How to Cite this paper?
APA-7 Style
Shang,
J., Lin,
H., Tian,
Y., Wu,
L. (2023). Effect of Toll-Like Receptor 4 on Angiotensin II-Induced Cardiac Hypertrophy in Mice. Trends in Medical Research, 18(1), 152-160. https://doi.org/10.3923/tmr.2023.152.160
ACS Style
Shang,
J.; Lin,
H.; Tian,
Y.; Wu,
L. Effect of Toll-Like Receptor 4 on Angiotensin II-Induced Cardiac Hypertrophy in Mice. Trends Med. Res 2023, 18, 152-160. https://doi.org/10.3923/tmr.2023.152.160
AMA Style
Shang
J, Lin
H, Tian
Y, Wu
L. Effect of Toll-Like Receptor 4 on Angiotensin II-Induced Cardiac Hypertrophy in Mice. Trends in Medical Research. 2023; 18(1): 152-160. https://doi.org/10.3923/tmr.2023.152.160
Chicago/Turabian Style
Shang, Junjun, Hailong Lin, Yuqing Tian, and Lin Wu.
2023. "Effect of Toll-Like Receptor 4 on Angiotensin II-Induced Cardiac Hypertrophy in Mice" Trends in Medical Research 18, no. 1: 152-160. https://doi.org/10.3923/tmr.2023.152.160

This work is licensed under a Creative Commons Attribution 4.0 International License.