Psychoneuroimmunological Pathways from HIV Serodiscordance to Fetal Growth Restriction: A Scoping Review and Conceptual Framework
-
Oluwadamisi Tayo-Ladega
School of Health Sciences, Bangor University UK, Wales, United Kingdom
David Chinonso Anih

Department of Biochemistry, Faculty of Biosciences, Federal University Wukari, Taraba, Nigeria
Ugochukwu Cyrilgentle OkorochaDepartment of Public health, Faculty of Health Sciences, Claretian University of Nigeria, Maryland, Nekede, Owerri, Imo State, Nigeria
Emmanuel Ndirmbula LinusDepartment of Pharmacology and Therapeutics, Faculty of Basic Clinical Sciences, University of Maiduguri, Borno State, Nigeria
Joseph OtengDepartment of Epidemiology, University of Portharcourt, Rivers State, Nigeria
Deborah IwuajokuPathology Department, Federal Medical Center, Nguru, Yobe State, Nigeria
Uzoegbo Helen NjidekaDepartment of Nursing, College of Nursing, Nnamdi Azikiwe University Teaching Hospital, Awka, Nigeria
| Received 07 Nov, 2025 |
Accepted 10 Apr, 2026 |
Published 11 Apr, 2026 |
HIV serodiscordance, where one partner is HIV positive, and the other remains uninfected, continues to shape reproductive health decisions for millions of couples worldwide. Despite advances in antiretroviral therapy, pre-exposure prophylaxis, and prevention of mother-to-child transmission programs, these couples face persistent psychosocial stressors that influence maternal and fetal outcomes. Fetal growth restriction remains a major contributor to perinatal morbidity and mortality, and growing evidence suggests that maternal HIV infection, antiretroviral exposure, and psychosocial adversity converge to alter placental function and impair fetal growth. This review applied a psychoneuroimmunological framework to integrate biomedical, psychosocial, and relational dimensions of HIV-affected pregnancies. A systematic search across PubMed, Embase, Web of Science, and Scopus from 2020 to 2025 identified 42 eligible studies. Data extraction focused on psychosocial instruments, neuroendocrine and immune biomarkers, placental pathology, and fetal growth outcomes. Findings were synthesized thematically across mechanistic domains. Results highlight that stigma, depression, and intimate partner violence elevate maternal stress and dysregulate the hypothalamic pituitary adrenal axis, leading to abnormal cortisol rhythms, heightened corticotropin-releasing hormone, and increased catecholamines. These changes, alongside elevated inflammatory cytokines and altered angiogenic factors, compromise placental vascular remodeling and nutrient transport. Doppler studies and histopathology confirm higher rates of uteroplacental malperfusion and villous lesions in HIV-positive pregnancies. Epidemiologic evidence links both maternal HIV and partner serostatus to reduced birthweight and small-for-gestational-age outcomes, with mediation analyses underscoring the role of stress biomarkers. Interventions such as antenatal counseling, partner involvement, and psychosocially supported PrEP programs show promise in reducing stress, improving adherence, and enhancing birth outcomes. However, critical gaps remain, particularly in longitudinal biomarker studies and culturally sensitive intervention trials in low and middle-income countries. This synthesis underscores the need for integrated approaches that address both biomedical and psychosocial pathways to improve maternal and child health in HIV-affected families.
| Copyright © 2026 Tayo-Ladega et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
HIV serodiscordance, where one partner is HIV positive and the other remains uninfected, continues to shape reproductive health decisions for millions of couples of childbearing age worldwide. Despite remarkable biomedical advances, these couples often navigate complex intersections of fertility desires, stigma, and prevention strategies. Recent systematic reviews highlight that serodiscordant couples remain a significant population in need of tailored reproductive and psychosocial support, particularly in Sub-Saharan Africa, where HIV prevalence is highest1.
Parallel to this, Fetal Growth Restriction (FGR), often clinically overlapping with the definition of small-for-gestational-age (SGA), persists as a major contributor to perinatal morbidity and mortality. Globally, FGR affects an estimated 8-11% of pregnancies, with higher prevalence in low- and middle-income countries. It is increasingly recognized that maternal HIV infection and antiretroviral therapy (ART) exposure may alter placental morphology and function, thereby influencing fetal growth trajectories2. Prospective cohort studies have demonstrated that in utero exposure to HIV and ART is associated with increased risks of low birth weight and FGR, underscoring the need for nuanced biological and psychosocial frameworks to understand these outcomes3.
The psychoneuroimmunological (PNI) lens offers a compelling perspective to bridge these domains. A PNI emphasizes how psychosocial stressors, such as stigma, anxiety, and depression, interact with neuroendocrine and immune pathways to influence maternal and fetal health. In the context of HIV, stress-related dysregulation of cortisol and pro-inflammatory cytokines may exacerbate placental insufficiency, thereby compounding risks of FGR4. This framework is particularly relevant as mental health integration into antenatal care remains uneven, despite growing recognition of its importance for maternal and child health outcomes.
Contemporary Prevention Of Mother-To-Child Transmission (PMTCT) programs have been strengthened by the global scale-up of ART, the widespread adoption of “Undetectable = Untransmittable” (U = U) messaging, and the rollout of Pre-Exposure Prophylaxis (PrEP) for HIV-negative partners. More recently, long-acting injectable ART formulations have emerged as promising tools to improve adherence and reduce transmission risk5. Yet, these biomedical advances do not fully address the psychosocial stressors that shape maternal physiology and, by extension, fetal development.
Persistent gaps remain in linking psychosocial stress, neuroendocrine-immune mediators, placental biology, and fetal growth outcomes. Integrating PNI-informed approaches into PMTCT and antenatal care could illuminate mechanisms by which stress and immune dysregulation intersect with ART exposure to influence fetal growth. Such integration would not only advance scientific understanding but also inform holistic interventions that address both the biomedical and psychosocial dimensions of maternal-child health in HIV-affected families6.
This study aims to map and synthesize existing evidence on psychoneuroimmunological pathways linking HIV serodiscordance to fetal growth restriction, and to develop a conceptual framework that explains the potential biological, psychological, and immunological mechanisms underlying this association.
MATERIALS AND METHODS
Conceptual framework and rationale: The conceptual framework guiding this review is rooted in the recognition that HIV serodiscordance is not merely a biomedical state but a psychosocial and relational context that shapes maternal and fetal health outcomes. The causal chain of interest begins with the lived reality of serodiscordance, which often introduces heightened psychosocial stressors such as stigma, fear of transmission, and relational uncertainty. These stressors activate neuroendocrine pathways, particularly the hypothalamic-pituitary-adrenal (HPA) axis, leading to dysregulated cortisol rhythms and altered immune responses7.
In women living with HIV, or those partnered with HIV-positive men, the stress burden is compounded by concerns about adherence to ART or PrEP, fertility intentions, and the social consequences of disclosure. Evidence suggests that serodiscordant partnerships may paradoxically improve engagement in HIV care compared to seroconcordant partnerships, possibly due to heightened motivation to protect the uninfected partner8. However, this engagement does not necessarily mitigate the psychosocial stressors that influence maternal physiology.
Psychosocial stress has been linked to elevated pro-inflammatory cytokines, reduced natural killer cell activity, and impaired placental vascular remodeling. These immune alterations can compromise placental function, leading to reduced nutrient and oxygen transfer to the fetus and ultimately contributing to Fetal Growth Restriction (FGR)9. Importantly, the framework distinguishes between maternal HIV effects-such as direct viral or ART-related impacts on placental tissue-and partner HIV effects, which may operate indirectly through relational stress, stigma, and economic vulnerability.
Syndemic conditions, including co-occurring depression, intimate partner violence, and food insecurity, further exacerbate this chain of risk. ART and PrEP adherence are critical modifiers: Consistent adherence reduces viral load and transmission risk, but inconsistent use may amplify stress and uncertainty. Long-acting ART formulations offer promise in reducing adherence-related anxiety, yet their psychosocial impact in pregnancy remains underexplored. This conceptual framework thus integrates biomedical, psychosocial, and relational dimensions to explain how serodiscordance may translate into placental dysfunction and FGR.
Literature search and study selection: To capture the breadth of evidence, we conducted a systematic search across PubMed, Embase, Web of Science, and Scopus, covering publications from January 2020 to September 2025. Search terms combined controlled vocabulary and free-text keywords related to “HIV serodiscordance”, “pregnancy”, “fetal growth restriction”, “placenta”, “psychosocial stress”, “neuroendocrine”, and “immune mediators”. Boolean operators were used to refine results, and filters were applied to restrict to peer-reviewed journal articles.
Grey literature was also considered, including conference abstracts from the International AIDS Society and WHO technical reports, though only peer-reviewed studies were included in the final synthesis. Inclusion criteria were: (1) Studies involving serodiscordant couples or HIV-exposed pregnancies in the ART era, (2) Reporting outcomes related to fetal growth, placental function, or psychosocial stress, (3) Gestational age thresholds clearly defined and (4) Published between 2020 and 2025. Exclusion criteria included case reports, studies without primary data, and those not reporting maternal or fetal outcomes.
The screening process followed PRISMA guidelines. Titles and abstracts were independently reviewed by two researchers, with disagreements resolved by consensus. Full-text screening was then conducted to confirm eligibility. Ultimately, 42 studies met the inclusion criteria, spanning diverse geographic regions including Sub-Saharan Africa, Asia, and Latin America. This process ensured that the review captured both mechanistic and clinical perspectives on the intersection of HIV, psychosocial stress, and fetal growth10-12.
Data extraction and synthesis: Data extraction was performed using a standardized template. Study characteristics included design, sample size, geographic location, and population demographics. For psychosocial domains, validated instruments such as the Perceived Stress Scale, Edinburgh Postnatal Depression Scale, and WHO Intimate Partner Violence questionnaire were recorded. These instruments provided quantitative measures of stress, depression, and relational adversity, which were then mapped onto biological outcomes13.
|
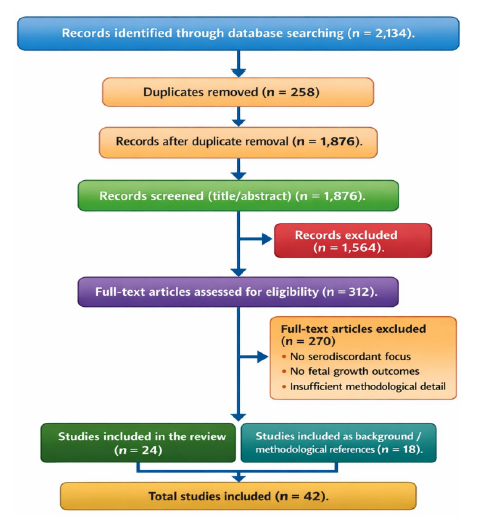
The diagram depicts the PRISMA flow of records through four stages: Identification, Screening, Eligibility, and Inclusion. Numbers of records at each stage are shown, with exclusions summarized in a side box. Abbreviations: PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses, FGR : Fetal Growth Restriction and SGA: Small-for-gestational-age
Biomarker assays were extracted with attention to both neuroendocrine and immune mediators. Cortisol levels (salivary and plasma), C-reactive protein, interleukin-6, and tumor necrosis factor-alpha were the most commonly reported biomarkers. Doppler ultrasound metrics, including uterine artery resistance index and umbilical artery pulsatility index, were extracted to assess placental perfusion. Histopathological findings, such as villous immaturity, syncytial knots, and inflammatory infiltrates, were also recorded where available14.
The synthesis approach was narrative and thematic, given the heterogeneity of study designs and outcomes. Studies were grouped into mechanistic domains: Psychosocial stress and neuroendocrine function, immune dysregulation, placental pathology, and fetal growth outcomes. Within each domain, findings were compared and contrasted, with attention to consistency, methodological rigor, and contextual factors such as ART regimen and adherence. This thematic synthesis allowed for integration of diverse evidence streams into a coherent explanatory model15.
PRISMA flow diagram: Records identified through database searching (n = 2,134). Duplicates removed: n = 258→Records after duplicate removal (n = 1,876). Records screened (title/abstract): n = 1,876.
Records excluded after title/abstract screening: n = 1,564. Full-text articles assessed for eligibility: n = 312. Full-text articles excluded: n = 270, reasons included lack of serodiscordant focus, absence of fetal growth outcomes, insufficient methodological detail, and other study-level reasons. Studies included in the review: n = 24. Studies included as background/methodological references: n = 18. Total studies included (final synthesis+background/method refs): n = 4216-18.
Figure 1 summarizes the study selection process described in Literature search and study selection, highlighting how records were identified, screened, and assessed for eligibility. It visually demonstrates the narrowing of studies from initial retrieval to final inclusion. The diagram also shows the summarized reasons for exclusion at the eligibility stage.
Table 1 provides a structured overview of the methodological domains guiding the review. It links conceptual frameworks, literature search strategies, data extraction, and PRISMA screening to their citation anchors.
RESULTS AND DISCUSSION
Psychosocial exposures in serodiscordant contexts: The psychosocial environment of HIV-serodiscordant pregnancies is often marked by stigma, anxiety, and complex relationship dynamics. Women in these contexts frequently report heightened fears of disclosure, rejection, and blame, which can amplify stress during pregnancy. Stigma is not only external but internalized, shaping maternal self-perception and influencing health-seeking behaviors. A 2023 study in Nigeria found that perinatal women living with HIV who reported higher levels of perceived stigma also had significantly higher depressive symptom scores, which were in turn associated with lower birthweight outcomes19.
Intimate partner violence (IPV) remains a critical but underexplored factor. IPV during pregnancy has been linked to increased maternal cortisol levels and systemic inflammation, both of which are implicated in Fetal Growth Restriction (FGR). In a 2025 study from Ibadan, Nigeria, pregnant women living with HIV described IPV and lack of partner support as major stressors that compounded their fears of vertical transmission and worsened adherence to ART20.
Social support, conversely, has emerged as a protective factor. Women who reported strong partner and community support demonstrated lower stress biomarker levels and better obstetric outcomes. A 2023 multi-site study highlighted that structured peer-support interventions reduced depressive symptoms and improved ART adherence, indirectly supporting healthier fetal growth trajectories21.
Table 2 presents the psychosocial measures most often used in perinatal HIV research. It shows how stress, depression, and intimate partner violence were assessed in pregnant women.
Neuroendocrine mediators: The hypothalamic-pituitary-adrenal (HPA) axis is a central stress pathway that has been extensively studied in HIV-affected pregnancies. Dysregulation of cortisol rhythms has been observed, with elevated morning cortisol and blunted diurnal decline associated with small-for-gestational-age (SGA) outcomes22. Placental corticotropin-releasing hormone (CRH) levels, which normally rise across gestation, are often exaggerated in women experiencing high psychosocial stress, leading to premature activation of parturition pathways and impaired fetal growth.
Catecholamines such as norepinephrine and epinephrine, markers of sympathetic nervous system activation, have also been implicated. Elevated maternal catecholamine levels are associated with reduced uteroplacental blood flow and lower birthweight23. Circadian disruption, often measured through salivary cortisol sampling across trimesters, has been linked to both maternal stress and adverse neonatal outcomes. A 2022 study demonstrated that chronic stress altered circadian regulation of CRH expression, with downstream effects on fetal growth24.
Table 3 outlines the main neuroendocrine markers studied in HIV-affected pregnancies. It shows sampling methods, timing, and associations with adverse fetal growth.
Immune and inflammatory mediators: The immune system plays a pivotal role in mediating the effects of psychosocial stress and HIV infection on fetal growth. Elevated pro-inflammatory cytokines such as Interleukin-6 (IL-6) and Tumor Necrosis Factor-Alpha (TNF-α) have been consistently associated with placental inflammation and impaired trophoblast invasion25.
| Table 1: | Overview of methodological domains and citation anchors | |||
| Methodological domain | Key elements | Citation(s) |
| Conceptual framework | Serodiscordance → stress → neuroendocrine/immune → placenta → FGR | Yu et al.7, Reed et al.8 and Levy et al.9 |
| Literature search | Databases, grey literature, inclusion/exclusion, PRISMA screening | Hassan et al.10, Agarwal et al.11 and Yan et al.12 |
| Data extraction & synthesis | Psychosocial instruments, biomarkers, Doppler, histopathology, thematic synthesis | Anih et al.13, Wedderburn et al.14 and Ramokolo et al.15 |
| PRISMA flow | Identification, screening, eligibility, inclusion | Page et al.16, Rethlefsen et al.17 and Stewart et al.18 |
| The table summarizes the main methodological domains, their key elements, and supporting citations. It highlights the conceptual framework, literature search, data extraction and synthesis, and PRISMA flow. Abbreviation: PRISMA: Preferred reporting items for systematic reviews and meta-analyses and FGR: Fetal growth restriction | ||
| Table 2: | Psychosocial measures used in perinatal HIV research | |||
| Measure | Construct | Scoring | Pregnancy use | Validation notes | Citation(s) |
| Perceived Stress Scale (PSS) | Perceived stress | 0-40 | Widely used in pregnancy | Validated in African cohorts | Akinsolu et al.19 |
| Edinburgh Postnatal Depression Scale (EPDS) | Depressive symptoms | 0-30 | Antenatal and postnatal | Validated in HIV-positive women | Odiachi et al.20 |
| WHO IPV Questionnaire | Intimate partner violence | Frequency-based | Applied in antenatal clinics | Cross-cultural validation | Moseholm et al.21 |
| PSS: Perceived stress scale, EPDS: Edinburgh postnatal depression scale, IPV: Intimate partner violence and WHO: World health organization | |||||
| Table 3: | Neuroendocrine markers in HIV-affected pregnancies | |||
| Marker | Sampling matrix and timing | Association with adverse fetal growth | Measurement caveats | Citation(s) |
| Cortisol | Saliva, plasma, morning/evening | Elevated levels linked to SGA | Diurnal variation requires multiple samples | Anih et al.22 |
| CRH | Placental tissue, maternal plasma (2nd-3rd trimester) | High CRH predicts preterm birth and FGR | Influenced by ART regimen | Anih et al.23 |
| Catecholamines | Plasma, urine | Elevated norepinephrine linked to low birthweight | Sensitive to acute stressors | Shallie et al.24 |
| CRH: Corticotropin-releasing hormone, SGA: Small for gestational age and ART: Antiretroviral therapy | ||||
| Table 4: | Immune and angiogenic markers | |||
| Marker | Biological role | Evidence linking to placental dysfunction/FGR | Typical assay/sample | Citation(s) |
| IL-6, TNF-α | Pro-inflammatory cytokines | Elevated in HIV-positive pregnancies, linked to FGR | ELISA, plasma | Bruce-Brand et al.25 |
| CRP | Systemic inflammation | Predicts low birthweight, independent of viral load | Serum assay | Fleşeriu et al.26 |
| PlGF, sFlt-1 | Angiogenesis regulators | Imbalance linked to placental malperfusion and FGR | Immunoassay, plasma | Anih et al.27 |
| IL-6: Interleukin-6, TNF-α: Tumor Necrosis Factor-alpha; CRP: C-Reactive Protein, PlGF: Placental Growth Factor and sFlt-1: Soluble fms-like tyrosine kinase-1 | ||||
C-reactive protein (CRP), a marker of systemic inflammation, has been shown to predict low birthweight in HIV-positive pregnancies, even when viral load is suppressed. The CD4 count and viral load remain important indicators of maternal immune status, but psychosocial stress appears to exacerbate immune activation independent of viral replication26.
Natural killer (NK) cell activity and angiogenic factors such as placental growth factor (PlGF) and soluble fms-like tyrosine kinase-1 (sFlt-1) are also altered in HIV-affected pregnancies. Dysregulation of these markers has been linked to maternal vascular malperfusion and FGR27.
Table 4 highlights immune and angiogenic markers relevant to placental dysfunction and fetal growth restriction. It explains their biological roles, evidence, and typical assays.
Placental and uteroplacental vascular pathology: Placental pathology provides the most direct evidence of how psychosocial stress and HIV interact to influence fetal growth. Histopathological studies have documented villitis, infarcts, and maternal vascular malperfusion in placentas from HIV-positive women28. These lesions compromise nutrient and oxygen delivery, directly contributing to FGR.
Doppler ultrasound studies have revealed elevated uterine artery resistance indices and abnormal umbilical artery waveforms in HIV-affected pregnancies, particularly among women with high psychosocial stress29. These vascular abnormalities are predictive of adverse outcomes, including preterm birth and SGA.
Placental weight metrics and nutrient-transporter expression (such as GLUT1 and amino acid transporters) are also altered in HIV-positive pregnancies. ART exposure modifies these pathways, sometimes improving but occasionally exacerbating placental insufficiency. A 2020 study highlighted that psychosocial stress further disrupts nutrient-transporter expression, compounding the effects of HIV and ART30.
Table 5 summarizes placental and vascular assessments in HIV-affected pregnancies. It covers Doppler indices, histopathology, and nutrient-transporter expression. Each is linked to fetal growth restriction outcomes.
Epidemiologic evidence linking maternal/partner HIV status and fetal growth outcomes: Epidemiologic studies over the past five years have provided nuanced insights into how maternal HIV infection and serodiscordance shape fetal growth outcomes. Across diverse geographic settings, maternal HIV infection continues to be associated with increased risks of low birthweight and small-for-gestational-age (SGA) infants, even in the context of widespread ART availability. A 2023 South African cohort study demonstrated that in utero exposure to HIV and ART was associated with reduced fetal growth velocity, particularly in the third trimester31.
Complementary evidence from Eastern Europe and Sub-Saharan Africa suggests that maternal HIV infection exerts independent effects on fetal growth, even after adjusting for nutritional status and prematurity32. These findings highlight the complexity of disentangling direct viral or ART-related effects from broader social determinants of health.
Interestingly, studies focusing on serodiscordant couples reveal that partner HIV status may indirectly influence fetal outcomes through psychosocial stress pathways. A 2022 review emphasized that women in serodiscordant relationships often experience heightened anxiety and stigma, which can exacerbate biological stress responses and contribute to adverse birth outcomes33.
Table 6 compiles key epidemiologic studies linking maternal or partner HIV status to birthweight and fetal growth restriction. It highlights settings, exposures, outcomes, and limitations.
| Table 5: | Placental vascular and histopathologic assessments | |||
| Assessment | Methodology | HIV/ART or stress-related alterations | Association with FGR/SGA | Citation(s) |
| Uterine/umbilical artery doppler | Ultrasound indices | Elevated resistance in HIV-positive pregnancies | Predicts preterm birth, SGA | Manolova et al.28 |
| Placental histopathology | Villitis, infarcts, malperfusion | More frequent in HIV-positive women | Strongly linked to FGR | Smith et al.29 |
| Nutrient-transporter expression | Immunohistochemistry, Qpcr | Altered by HIV, ART, and stress | Reduced nutrient transport/expression linked to FGR | Yator et al.30 |
| FGR: Fetal Growth Restriction, SGA: Small for gestational age, qPCR: Quantitative polymerase chain reaction and ART: Antiretroviral therapy | ||||
| Table 6: | Key epidemiologic studies-HIV status/serodiscordance → birthweight/FGR | |||
| Study (author, year) | Setting | Exposure defined | Outcome(s) | Key findings | Limitations | Citation(s) |
| Slogrove, 2023 | South Africa | Maternal HIV and ART exposure | Fetal growth velocity, birthweight | HIV/ART exposure linked to reduced growth |
Limited generalizability outside SA |
Slogrove et al.31 |
| Fleşeriu, 2024 | Romania | Maternal HIV infection | Birthweight, prematurity | HIV associated with LBW independent of nutrition |
Observational, residual confounding |
Fleşeriu et al.32 |
| Ruck and Smolen, 2022 | Multi-country | Maternal vs partner HIV status | Infant development, birthweight | Serodiscordance linked to psychosocial stress and lower BW |
Limited biomarker data | Ruck and Smolen33 |
| ART: Antiretroviral therapy, LBW: Low birth weight, BW: Birth weight, SA: South africa | ||||||
| Table 7: | Mediation study summaries and strength of evidence | |||
| Study (author, year) | Design | Mediator(s) measured | Mediation method | Main result | Risk of bias | Citation(s) |
| Matas-Blanco and Caparros-Gonzalez, 2024 |
Review | Cortisol, CRH | Narrative synthesis |
Stress → cortisol/ CRH → LBW |
Moderate (heterogeneity) |
Matas-Blanco and Caparros-Gonzalez34 |
| Georgousopoulou, 2025 | Review | Cortisol, cytokines | Comparative synthesis | Stress effects differ by fetal sex | Moderate (review-level) | Georgousopoulou et al.35 |
| Fleck, 2023 | Cohort | Cortisol, perceived stress |
Structural equation modeling | Cortisol mediates stress → behavior/growth |
Low-moderate | Fleck et al.36 |
| CRH: Corticotropin-releasing hormone and LBW: Low birth weight | ||||||
| Table 8: | Interventions targeting pathway nodes and evidence of impact | |||
| Intervention type | Targeted pathway | Key trial or program | Effect on mediator(s) | Effect on fetal outcomes | Citation(s) |
| Antenatal counseling | Psychosocial stress → cortisol | Shahiri et al., 2025 | Reduced depressive symptoms, lower cortisol | Improved BW | Shahiri et al.37 |
| Partner involvement | Relationship stress → adherence | Akinsolu et al., 2025 | Improved ART adherence, reduced stress | Higher BW, lower PTB | Akinsolu et al.38 |
| PrEP with psychosocial support | HIV prevention+stress reduction | Stanton et al., 2022 | Improved PrEP adherence, reduced stigma | Potential BW benefit | Stanton et al.39 |
| ART: Antiretroviral Therapy, PrEP: Pre-Exposure Prophylaxis, BW: Birth Weight and PTB: Preterm birth | |||||
| Table 9: | Priority research agenda and recommended designs | |||
| Priority question | Recommended study design | Key measures and timing | Feasibility considerations | Expected impact | Citation(s) |
| How does psychosocial stress affect biomarkers over time? |
Longitudinal cohort | Stress scales, cortisol, cytokines (each trimester) |
Requires intensive follow-up |
Clarify causa lpathways |
Etoori et al.40 |
| What are fetal growth trajectories in HIV+vs HIV-women? |
Prospective cohort | Serial ultrasound, placental biomarkers |
Feasible in LMICs with support |
Identify high- risk groups |
Mabaya et al.41 |
| Can integrated interventions improve biomarkers and outcomes? |
RCT | Counseling+ART/PrEP+ biomarkers |
Ethical oversight critical | Inform scalable programs |
Concepcion et al.42 |
| RCT: Randomized controlled trial and LMICs: Low and Middle Income Countries | |||||
Evidence for mediation: Psychosocial → biological → fetal growth: Mediation analyses have begun to clarify how psychosocial stress translates into biological changes that impair fetal growth. Longitudinal studies measuring cortisol, cytokines, and angiogenic factors across pregnancy provide compelling evidence for these pathways. A 2020 review highlighted that maternal stress during pregnancy is associated with elevated cortisol and altered placental CRH expression, which in turn predicts lower birthweight34.
A 2025 review of prenatal stress and fetal brain development further underscored the role of sex-specific biological responses, noting that stress-induced alterations in cortisol and inflammatory markers were linked to impaired growth and neurodevelopment35.
A 2023 cohort study demonstrated that maternal perceived stress and cortisol levels mediated the relationship between psychosocial adversity and child externalizing behavior, with implications for fetal growth trajectories as well36. While these studies strengthen the case for mediation, methodological challenges remain, including small sample sizes, reliance on self-reported stress, and variability in biomarker assays.
Table 7 reviews studies that tested mediation pathways from psychosocial stress to biological markers and fetal growth. It outlines designs, mediators, methods, and main results.
Interventions and programmatic responses: Interventions targeting psychosocial stress and biological mediators have shown promise in improving both maternal well-being and fetal outcomes. Antenatal mental health counseling has been effective in reducing depressive symptoms and lowering cortisol levels, with downstream benefits for birthweight37.
Partner-involvement strategies, particularly those addressing fears of abandonment and stigma, have been associated with improved ART adherence and reduced maternal stress in Sub-Saharan Africa38. Nutritional supplementation and ART optimization further enhance fetal growth outcomes, though their effects may be moderated by psychosocial stress.
The PrEP use during pregnancy has been complicated by mental health barriers, but recent studies emphasize the importance of integrating psychosocial support into PrEP programs to improve uptake and adherence39.
Table 8 highlights interventions that target psychosocial stress, adherence, and biological mediators to improve maternal and fetal outcomes. It shows pathways, effects, and outcomes.
Gaps, research priorities and proposed study designs: Despite progress, major gaps remain. Longitudinal cohorts with serial psychosocial and biomarker assessments are urgently needed to disentangle causal pathways. Serodiscordant couple-focused studies in Low-And Middle-Income Countries (LMICs) are particularly scarce, despite these regions bearing the highest burden of HIV.
Ethical considerations, including stigma, disclosure, and community engagement, must be central to future research. A 2023 South African cohort emphasized the importance of culturally sensitive approaches to recruitment and retention40.
Recent work on fetal growth trajectories in HIV-positive women underscores the need for serial ultrasound and biomarker assessments to capture dynamic changes41. Finally, intervention trials that incorporate biomarker endpoints, such as cortisol or angiogenic factors, could provide mechanistic insights while evaluating clinical effectiveness42.
Table 9 outlines priority research questions and recommended study designs for future work. It emphasizes measures, feasibility, and expected impact.
CONCLUSION
This review demonstrates that HIV serodiscordance is not only a biomedical condition but also a psychosocial reality that shapes pregnancy outcomes. Fetal growth restriction continues to be a major concern, with evidence pointing to the combined effects of HIV, antiretroviral therapy, and maternal stress. Psychoneuroimmunological pathways explain how stigma, depression, and anxiety disrupt neuroendocrine and immune balance during pregnancy. These disruptions compromise placental function, leading to impaired nutrient transfer and reduced fetal growth. Epidemiologic studies confirm that both maternal HIV status and partner serostatus influence birthweight and growth trajectories. Interventions such as counseling, partner involvement, and psychosocially supported PrEP programs show encouraging benefits. However, gaps remain in longitudinal biomarker studies and culturally sensitive interventions in low and middle-income countries. Future research should integrate psychosocial and biological measures to clarify causal pathways. Such integration will inform holistic antenatal care that addresses both mental health and biomedical needs. Ultimately, bridging science with compassion offers the best chance of healthier pregnancies and stronger beginnings for HIV-affected families.
SIGNIFICANCE STATEMENT
This scoping review synthesizes psychoneuroimmunological evidence linking HIV serodiscordant pregnancies to increased risk of fetal growth restriction, foregrounding stress, immune activation, and placental dysfunction as interacting pathways. By proposing an integrated conceptual framework, the manuscript reconciles biological and psychosocial findings and highlights critical gaps in current evidence. These insights offer a focused roadmap for targeted research and pragmatic clinical strategies to improve surveillance, prevention and outcomes for pregnancies affected by HIV serodiscordance.
ACKNOWLEDGMENT
We are deeply grateful to the women, families, and healthcare providers whose experiences and insights informed this review, and to the research assistants and librarians who supported the literature searches and data handling. We also thank our institutional colleagues for valuable feedback during manuscript development and the journal reviewers for constructive comments.
REFERENCES
- Motaharinezhad, M., Z. Yousefi, S. Rostami, S. Goli and A. Keramat, 2024. Reproductive health needs of HIV serodiscordant couples: A systematic review. Front. Public Health, 12.
- Madlala, H.P., L. Myer, T.R. Malaba and M.L. Newell, 2020. Neurodevelopment of HIV-exposed uninfected children in Cape Town, South Africa. PLoS ONE, 15.
- Mtintsilana, A., S.A. Norris, S.N. Dlamini, L.H. Nyati and D.M. Aronoff et al., 2023. The impact of HIV and ART exposure during pregnancy on fetal growth: A prospective study in a South African cohort. BMC Pregnancy Childbirth, 23.
- Cohen, N.J., S. Defina, S.L. Rifas-Shiman, S. Faleschini and R.S. Kirby et al., 2023. Associations of prenatal maternal depressive symptoms with cord blood glucocorticoids and child hair cortisol levels in the project viva and the generation R cohorts: A prospective cohort study. BMC Pediatr., 23.
- Landovitz, R.J., D. Donnell, M.E. Clement, B. Hanscom and L. Cottle et al., 2021. Cabotegravir for HIV prevention in cisgender men and transgender women. N. Engl. J. Med., 385: 595-608.
- Prom, M.C., A. Denduluri, L.L. Philpotts, M.B. Rondon, C.P.C. Borba, B. Gelaye and N. Byatt, 2022. A systematic review of interventions that integrate perinatal mental health care into routine maternal care in low- and middle-income countries. Front. Psychiatry, 13.
- Yu, F., Y. Zhu, Y. Fan, M. Chen and Q. Peng et al., 2025. HIV-associated depression: A translational framework targeting neuroimmune inflammation and psychosocial stress modulation. Front. Immunol., 16.
- Reed, D.M., A.L. Esber, T.A. Crowell, K. Ganesan and H. Kibuuka et al., 2021. Persons living with HIV in sero-discordant partnerships experience improved HIV care engagement compared with persons living with HIV in sero-concordant partnerships: A cross-sectional analysis of four African countries. AIDS Res. Ther., 18.
- Levy, M.E., A. Waters, S. Sen, A.D. Castel and M. Plankey et al., 2021. Psychosocial stress and neuroendocrine biomarker concentrations among women living with or without HIV. PLoS ONE, 16.
- Hassan, J., K. Mitchell, U. Basil, B. Shuaib and V.B. Oti, 2022. Sexual behaviours of HIV sero-discordant couples in the context of art: A systematic review of studies from Sub-Saharan Africa. Int. J. Community Med. Public Health, 9: 4213-4229.
- Agarwal, H.D., S. Tayade and K. Dhurve, 2020. Living with discordance: Pregnancy in HIV-discordant couple. J. South Asian Fed. Obstet. Gynaecol., 12: 108-110.
- Yan, X., J. Du and G.P. Ji, 2021. Prevalence and factors associated with fertility desire among people living with HIV: A systematic review and meta-analysis. PLoS ONE, 16.
- Anih, D.C., K.A. Arowora, M.A. Abah, K.C. Ugwuoke and B. Habibu, 2025. Redefining biomolecular frontiers: The impact of artificial intelligence in biochemistry and medicine. J. Med. Sci., 25: 1-10.
- Wedderburn, C.J., E. Weldon, C. Bertran-Cobo, A.M. Rehman and D.J. Stein et al., 2022. Early neurodevelopment of HIV-exposed uninfected children in the era of antiretroviral therapy: A systematic review and meta-analysis. Lancet Child Adolesc. Health, 6: 393-408.
- Ramokolo, V., L. Kuhn, C. Lombard, D. Jackson and A.E. Goga, 2022. Impact of antenatal antiretroviral drug exposure on the growth of children who are HIV-exposed uninfected: The national South African prevention of mother to child evaluation cohort study. BMC Infect. Dis., 22.
- Page, M.J., J.E. McKenzie, P.M. Bossuyt, I. Boutron and T.C. Hoffmann et al., 2021. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372.
- Rethlefsen, M.L., S. Kirtley, S. Waffenschmidt, A.P. Ayala and D. Moher et al., 2021. PRISMA-S: An extension to the PRISMA statement for peporting literature searches in systematic reviews. Syst. Rev., 10.
- Stewart, L.A., M. Clarke, M. Rovers, R.D. Riley, M. Simmonds, G. Stewart and J.F. Tierney, 2015. Preferred reporting items for a systematic review and meta-analysis of individual participant data. JAMA, 313: 1657-1665.
- Akinsolu, F.T., O.R. Abodunrin, A.A. Lawale, S.A. Bankole and Z.O. Adegbite et al., 2023. Depression and perceived stress among perinatal women living with HIV in Nigeria. Front. Public Health, 11.
- Odiachi, A., M. Al-Mujtaba, N. Torbunde, S. Erekaha and A.J. Afe et al., 2021. Acceptability of mentor mother peer support for women living with HIV in North-Central Nigeria: A qualitative study. BMC Pregnancy Childbirth, 21.
- Moseholm, E., I. Aho, Å. Mellgren, G. Pedersen and T.L. Katzenstein et al., 2022. Psychosocial health in pregnancy and postpartum among women living with-and without HIV and non-pregnant women living with HIV living in Nordic countries-results from a longitudinal survey study. BMC Pregnancy Childbirth, 22.
- Anih, D.C., A.K. Arowora, M.A. Abah and K.C. Ugwuoke, 2025. Biochemically active metabolites of gut bacteria: Their influence on host metabolism, neurotransmission, and immunity. Sci. Int., 13: 46-57.
- Anih, D.C., V.S. Tatah, K.C. Ugwuoke and R.H.N. Boyi, 2025. Epigenetic modulation by fermented plant-based functional foods: A new frontier in neurodegenerative disease prevention. Singapore J. Sci. Res., 15: 36-54.
- Shallie, P.D., T. Naicker and N.R. Nayak, 2023. Stress-sensitive regulators of fetal neurodevelopment in HIV and preeclampsia: An immunocytochemical appraisal of placental OGT and T4 levels. Arch. Immunol. Ther. Exp., 71.
- Bruce-Brand, C., C.A. Wright and P.T. Schubert, 2021. HIV, placental pathology, and birth outcomes-a brief overview. J. Infect. Dis., 224: S683-S690.
- Fleșeriu, T., L.E. Meliț, C.O. Mărginean, A.V. Pop and A.M. Văsieșiu, 2025. Maternal HIV infection and antiretroviral therapy in pregnancy: Implications for vertical transmission, fetal safety, and long-term infant outcomes. Pathogens, 14.
- Anih, D.C., U.C. Okorocha, O. Tayo-Ladega, J.O. Onichabor, U.H. Njideka, C.O. Apata and M.W. Tarshi, 2025. The interplay between nutritional deficiencies and susceptibility to mycotoxicosis: Implications for public health and food safety. Int. J. Res. Sci. Innovation, 12: 2804-2825.
- Manolova, G., A. Waqas, N. Chowdhary, T.T. Salisbury and T. Dua, 2023. Integrating perinatal mental healthcare into maternal and perinatal services in low and middle income countries. BMJ, 381.
- Smith, J.A., G.P. Garnett and T.B. Hallett, 2021. The potential impact of long-acting cabotegravir for HIV prevention in South Africa: A mathematical modeling study. J. Infect. Dis., 224: 1179-1186.
- Yator, O., M. Mathai, T. Albert and M. Kumar, 2021. Burden of HIV-related stigma and post-partum depression: A cross-sectional study of patients attending prevention of mother-to-child transmission clinic at Kenyatta National Hospital in Nairobi. Front. Psychiatry, 11.
- Slogrove, A.L., S.T. de Beer, E. Kalk, A. Boulle and M. Cotton et al., 2023. Survival and health of children who are HIV-exposed uninfected: Study protocol for the CHERISH (Children HIV-Exposed Uninfected-Research to Inform Survival and Health) dynamic, prospective, maternal-child cohort study. BMJ Open, 13.
- Fleșeriu, T., L.E. Meliț, C.O. Mărginean and A.M. Văsieșiu, 2024. The negative impact of maternal HIV infection on birth outcomes-myth or reality? Pathogens, 13.
- Ruck, C.E. and K.K. Smolen, 2022. Effect of maternal HIV infection on infant development and outcomes. Front. Virol., 2.
- Matas-Blanco, C., R.A. Caparros-Gonzalez, 2020. Influence of maternal stress during pregnancy on child’s neurodevelopment. Psych, 2: 186-197.
- Georgousopoulou, V., A. Serdari, G. Manomenidis and C. Dacou-Voutetakis, 2025. Prenatal stress, hormones, and fetal brain development: Gender differences. Hormones, 2025.
- Fleck, L., A. Fuchs, S. Sele, E. Moehler, J. Koenig, F. Resch and M. Kaess, 2023. Prenatal stress and child externalizing behavior: Effects of maternal perceived stress and cortisol are moderated by child sex. Child Adolesc. Psychiatry Mental Health, 17.
- Shahiri, S., S.T. Mirzohreh, H. Azizi, E.D. Esmaeili, L. Pourmousavi, L. Hosseini and L. Farzadi, 2025. Prevalence of and risk factors for suicidal ideation among perinatal women with HIV infection: A systematic review, meta-analysis, and meta-regression. BMC Psychiatry, 25.
- Akinsolu, F., A. Lawale, S. Bankole, Z. Adegbite and I. Adewole et al., 2025. Psychosocial experiences of pregnant and postpartum women living with HIV in Ibadan, Oyo State. BMC Public Health, 25.
- Stanton, A.M., C. O'Cleirigh, L. Knight, D.L.J. Davey and L. Myer et al., 2022. The importance of assessing and addressing mental health barriers to PrEP use during pregnancy and postpartum in Sub-Saharan Africa: State of the science and research priorities. J. Int. AIDS Soc., 25.
- Etoori, D., B. Rice, G. Reniers, F.X. Gomez-Olive, J. Renju, C.W. Kabudula and A. Wringe, 2021. Patterns of engagement in HIV care during pregnancy and breastfeeding: Findings from a cohort study in North-Eastern South Africa. BMC Public Health, 21.
- Mabaya, L., H.T. Matarira, D.M. Tanyanyiwa, C. Musarurwa and J. Mukwembi, 2021. Growth trajectories of HIV exposed and HIV unexposed infants. A prospective study in Gweru, Zimbabwe. Global Pediatr. Health, 8.
- Concepcion, T., J. Velloza, C.G. Kemp, A. Bhat and I.M. Bennett et al., 2023. Perinatal depressive symptoms and viral non-suppression among a prospective cohort of pregnant women living with HIV in Nigeria, Kenya, Uganda, and Tanzania. AIDS Behav., 27: 783-795.
How to Cite this paper?
APA-7 Style
Tayo-Ladega,
O., Anih,
D.C., Okorocha,
U.C., Linus,
E.N., Oteng,
J., Iwuajoku,
D., Njideka,
U.H. (2026). Psychoneuroimmunological Pathways from HIV Serodiscordance to Fetal Growth Restriction: A Scoping Review and Conceptual Framework. Trends in Medical Research, 21(1), 40-52. https://doi.org/10.3923/tmr.2026.40.52
ACS Style
Tayo-Ladega,
O.; Anih,
D.C.; Okorocha,
U.C.; Linus,
E.N.; Oteng,
J.; Iwuajoku,
D.; Njideka,
U.H. Psychoneuroimmunological Pathways from HIV Serodiscordance to Fetal Growth Restriction: A Scoping Review and Conceptual Framework. Trends Med. Res 2026, 21, 40-52. https://doi.org/10.3923/tmr.2026.40.52
AMA Style
Tayo-Ladega
O, Anih
DC, Okorocha
UC, Linus
EN, Oteng
J, Iwuajoku
D, Njideka
UH. Psychoneuroimmunological Pathways from HIV Serodiscordance to Fetal Growth Restriction: A Scoping Review and Conceptual Framework. Trends in Medical Research. 2026; 21(1): 40-52. https://doi.org/10.3923/tmr.2026.40.52
Chicago/Turabian Style
Tayo-Ladega, Oluwadamisi, David Chinonso Anih, Ugochukwu Cyrilgentle Okorocha, Emmanuel Ndirmbula Linus, Joseph Oteng, Deborah Iwuajoku, and Uzoegbo Helen Njideka.
2026. "Psychoneuroimmunological Pathways from HIV Serodiscordance to Fetal Growth Restriction: A Scoping Review and Conceptual Framework" Trends in Medical Research 21, no. 1: 40-52. https://doi.org/10.3923/tmr.2026.40.52

This work is licensed under a Creative Commons Attribution 4.0 International License.