Implementation of the WHO STEPS Approach for NCD Risk Factor Surveillance in Rural Communities: Challenges, Adaptations, and Outcomes
-
Agoro, Oviemova Nathan
Department of Public Health, Faculty of Health Sciences, Bayelsa Medical University, Yenagoa, Bayelsa State, Nigeria
Osom Alexanda Lott OnyeucheDepartment of Obstetrics and Gynaecology, AI Gurayat General Hospital, Kingdom of Saudi Arabia
| Received 15 Apr, 2025 |
Accepted 20 Jun, 2025 |
Published 21 Jun, 2025 |
Background and Objective: Non-Communicable Diseases (NCDs) such as cardiovascular diseases, diabetes, and cancer present a growing global health challenge, particularly in low- and middle-income countries. This study aims to evaluate the implementation, challenges, and contributions of the WHO STEPS framework in facilitating national NCD surveillance and informing public health strategies. Materials and Methods: This descriptive study reviewed the implementation of the WHO STEPS surveys across more than 129 countries over the past decade. Emphasis was placed on the integration of mHealth technologies and the involvement of Community Health Workers (CHWs) to overcome infrastructural and cultural barriers. Data sources included national STEPS reports and WHO documentation. Thematic analysis was used to assess patterns in data usage, implementation challenges, and policy outcomes. Results: The STEPS framework successfully generated standardized, country-specific data critical for NCD monitoring and control. Participation included over 129 countries, with improvements in data quality and accessibility observed through the incorporation of mHealth tools and CHW training. These efforts enhanced survey reach, especially in rural and resource-constrained settings. The data informed national action plans and guided targeted interventions. Despite persistent challenges in healthcare infrastructure and logistics, the methodology proved adaptable and scalable across diverse contexts. Conclusion: The WHO STEPS framework has significantly contributed to global NCD surveillance, enabling countries to formulate evidence-based health policies. While challenges remain, particularly in under-resourced areas, the incorporation of digital tools and community-based approaches has enhanced its effectiveness. Future success will depend on continued international support, inter-country data-sharing, and adaptive strategies to sustain and expand NCD prevention efforts globally.
| Copyright © 2025 Nathan and Onyeuche. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Implementing the WHO STEPS approach for Non-Communicate Diseases (NCDs) risk factor surveillance in rural communities is crucial in shedding light on how to overcome health disparities, especially in low-resource settings. The World Health Organization (WHO) initiated the STEP wise Approach to Surveillance (STEPS) methodology to provide information on behavioural, physical, and biochemical risk factors so that policymakers can identify and reduce the increasing burden of Non-Communicable Diseases (NCDs), including cardiovascular diseases, diabetes and cancers. While it is still viable, several issues come along with the implementation of this approach in such a context since it faces logistical, cultural, and infrastructural drawbacks in rural areas. In this paper, information related to the problems faced, changes made to counter them, and their effects are hereby presented in this part of the work.
Chronic diseases are prevalent, and they are worse among the rural populace1. Some of the identifying factors that define the health services delivery issues in rural places include inadequate provision of health assets, information on health, and preventive measures against diseases2. Despite recognizing the WHO STEPS as a solution for assessing the risk factors of NCDs in such neglected regions, its application has revealed numerous barriers. Another risk is the shortage of well-trained personnel in the rural health facilities to undertake comprehensive surveys and assessments; all this distorts data quality and reliability3. In addition to that, there are issues of poor transport network and time-to-time interruptions in the internet connection during data collection, which makes data integration into the national health system a challenge4.
These new challenges have, therefore, rendered adaptation strategies an absolute necessity. To address the above capacity challenge, researchers and health authorities have introduced innovation in addressing the challenge through pre-service and in-service training of CHWs for data acquisition and dissemination5. In some regions of the world, mobile applications have been adopted to improve6. Although the current sections are beneficial in enhancing coverage of the WHO STEPS approach7, they require financial support and training to continue their operations8. Logistical solutions must be combined with cultural understanding in the development of surveys as well as in the analysis of the results. There are reasons to believe that rural populations can have certain culturally-relative beliefs about the risk factors or involvement in health research9.
This adaptation of the WHO STEPS methodology has thus also given insights into the broader issues of the implementation of the prevention of NCDs in the policy of public health in rural areas. The development of studies on STEPS applications in some countries like India and Rwanda demonstrates the fact that the country and city contexts have shown benefits of the STEPS approach; nevertheless, completely different conditions characteristic of rural areas demand essential transformations of the fundamental methodology10,11. Some of the interventions include carrying out mobile-based surveys and modifications of risk factors that can be understood by illiterate peasants12. This is not without disadvantages; for example, there is reduced depth and scope of data gathering that may affect the soundness of the data used in making policies13.
In spite of these challenges, there have been several accomplishments due to the use of the STEPS model in rural areas. For example, a community-based survey in India where implementation was done through the use of Community Health Workers led to an increased response rate and precise identification of the level of hypertension and diabetes in the community14. These inputs helped in calling for intended measures, for example adequate supply of drugs and health literature. In addition, the STEPS approach in the Rwanda and South Africa developed the equation of increased risk factors that include smoking patterns, and diets and have incorporated these findings into the national health master plans for intervention12. The evidence shows that, starting with necessary modifications, the STEPS approach can be a more efficient way of NCD surveillance in rural populations.
This paper identifies several implications for the implementation of the STEPS model, a well-articulated and comprehensive model for NCD risk factor surveillance established by the WHO. Consequently, solutions have to fit the rural paradigm while the right checks and balances need to be put in place so as not to cross the threshold into a whole new level of indifference. By focusing on enhancing local capacity and tying the private sector into a stronger nautical, the STEPS glycogen can be the foundation for surveillance and prevention of NCDs in rural civilization and contribute towards a better quality of living in numerous circadian global communities.
The purpose of this study is to identify the challenges that were experienced in the process of implementing the WHO STEPS approach within the rural setting, mainly concerning the issues of logistics, culture, and capabilities of the relevant healthcare institutions. It also attempts to find out how these challenges were addressed, especially by advancing technologies as well as training CHWs. The strength of the study is thus to assess modifications that have been made to these systems, especially the impact of such adaptations on the data quality of NCD risk factors surveillance and the impact on policy formulation and health interventions.
MATERIALS AND METHODS
Study area: This study was conducted between January, 2024 and February, 2025 in the Eight Local Government Areas of Bayelsa State as a primary location. However, secondary data were harvested from verifiable online platforms. Bayelsa State is one of the 36 states created in 1996 and is bounded by the Rivers and Delta States of Nigeria13-17.
STEPS framework overview: The WHO STEPS framework is developed under the concept that surveillance systems should include standardized data collection, but also provide adequate flexibility to ensure adaptation in different country contexts and settings15. Such flexibility accommodates the framework to function in low-resource as well as more advanced situations. One of the components central to the STEPS framework is acute and chronic risk-factor assessments that can be more detailed if time allows, so that data can be made more comparable between countries16.
Step 1
Collected behavioral and demographic data: The STEPS process gathers data on demographics and interviews individuals about their behavioral risk factors, such as tobacco use and screening for alcohol consumption, while assessing their diet and activity levels in step one17. This step also entails recording data on the history of NCDs, including hypertension, diabetes, cardiovascular diseases, and recommendations related to the control of NCDs2. These reports are primarily based on self-reports to provide information on behaviors that lead to the occurrence of NCDs among individuals18.
Step 2
Physical measurements: Take measurements to get some important health numbers. These include measuring Body Mass Index (BMI), waist circumference, and blood pressure, which are integral to identifying obesity and hypertension15. These physical indicators serve as significant markers in evaluating the risk factors related to cardiovascular diseases and diabetes9.
Step 3
Biochemical assessment: Step 3 concerns biochemical measurements, including fasting blood glucose, total cholesterol, and urinary sodium. Identify these biomarkers, which can identify biochemical risk factors for NCDs like diabetes and heart disease, and are usually taken at a local health facility or clinic. This latter stage is critical for validating the prevalence of NCD risk factors at a more physiological level, to provide an accurate health profile of the population.
Core and expanded modules: Each of the steps in the STEPS framework calls for countries to concentrate on the core elements of data collection, and that these represent the most critical risk factors. Nevertheless, nations with the resources will also decide to integrate “enhanced” modules for a more in-depth assessment of specific risk factors15. These expanded items may encompass more behaviour risk factors, such as in-depth questions on tobacco use or even anthropometric measures, such as hip circumference. This step also permits more biochemical measures, for example, triglycerides and High-Density Lipoprotein (HDL) cholesterol levels9. Additionally, the framework provides optional modules for other topics, such as mental health, oral health, and sexual and reproductive health, which may be included depending on local health priorities17.
Revisions and adaptation of STEPS instrument: The STEPS tool continues to be revised with new information on NCD risk factors and to ensure surveys are relevant to the current challenges in health18. The recent iterations have widened the scope to six important risk-factor objectives, along with one health systems target from the Global Monitoring Framework, which increases its utility for monitoring the most significant risk determinants of NCDs15.
Sampling methodology: The STEPS surveys are cross-sectional, population-based household repeat surveys. In most countries, multistage cluster sampling is employed to achieve a nationally representative sample of men and women aged 18-69 years. In contrast, in smaller or better-resourced countries, investigators may have employed an alternative approach (e.g., simple random sampling or census-based)16. The 5,000 to 6,000 participants are included in the survey, although this sample size is based on power estimates for age- and gender-specific estimates17.
Fieldwork implementation: The STEPS surveys are conducted through fieldwork, with trained interviewers surveying randomly selected households in face-to-face interviews. The participants also self-report data on behavioural risk factors, and blood pressure, Body Mass Index (BMI), and other physical measurements are obtained. Visiting local clinics or health centres for biochemical assessments is common15. The collection of this data has been made easier with the implementation of eSTEPS, a digital device. The eSTEPS does away with paper-based surveys and provides real-time error checking, participant selection, as well as automated skip patterns in questionnaires, making them more efficient and accurate18.
eSTEPS for data collection: By implementing eSTEPS, a full software suite developed for handheld PCs, we observed a significant improvement in the quality of data collected. The eSTEPS automatically selects participants, transfers information to the survey, error checks, copies data, and performs many of the functions required for a new survey to be completed, allowing for significantly shorter report completion times. In 2015, eSTEPS was extended to encompass mobile devices such as tablets and smartphones, which would allow for more flexibility when conducting surveys in diverse languages and environments17. Technological innovation has facilitated the implementation of STEPS in a variety of geographical settings, particularly low-resource settings, where conventional data collection is difficult15.
Coordination of STEPS surveys: The STEPS surveys are generally conducted with coordination at the national level led by health ministry officials and with local technical partners providing collaborative support19. Collaborative efforts of this kind allow the smooth running of surveys (in particular, but not limited to) in low and middle-income countries where there might be resource constraints. Most ministries of health are responsible for the finances of these surveys, distributing funds for local activities and logistical expenditures related to the survey. Quite often, these national authorities may even receive further funding from international donors20.
Resourcing for STEPS surveys: The STEPS surveys are predominantly funded by national governments, with the World Health Organization (WHO) providing essential resources. The WHO deploys technical devices like blood pressure measuring devices, small initial funds, and connections to possible international benefactors to help in survey implementation21. This is critical support for countries that may not have the resources in place to conduct the surveys on their own. The WHO further assists the surveys by providing them with the required tools for collecting quality health data that is so critical in policy formulation.
Technical support from WHO and partners: According to the development of STEPS, technical assistance can be provided from the WHO headquarters, regional offices, and various country-specific teams. This involves accompanying in various aspects of surveying, beginning from survey design up to survey data processing22. It also cooperates with numerous other technical non-governmental, and governmental organizations to help in the conduct of the WHO survey to ensure appropriate methods of data collection and reporting are upheld. There are several functions of training workshops depending on the stages of the survey that they are conducted, including a collection of data, analysis, and report writing23,24.
Available tools and resources: Many STEPS surveys have been completed worldwide because WHO and other partners provide numerous tools and resources for the implementation of STEPS surveys. It consists of the updated STEPS Manual for the survey, containing clear protocols and information on survey design, obtaining ethical clearances, and surveying19. This element increases survey access to such supports as sample size calculators and data collection forms for planning and collecting high-quality data for survey teams. It also provides data analysis programmes for several statistical packages so that the assembled data may be effectively analysed24.
Training and workshops: The WHO oversees the quality and consistency of STEPS surveys, holding training workshops at each step of the survey process. These workshops are facilitated via the planning, data collection and analysis, and reporting phases20. The purpose of these workshops is to expand and subtly graze the capacity of National Health systems to routinely employ survey methodology. More broadly, it ensures health professionals remain up to date with current survey methods and technology and can adapt to changing health environments.
RESULTS AND DISCUSSION
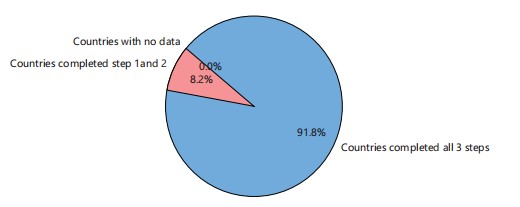
The data on the countries that completed the three programs of the Stepwise Approach to Surveillance (STEPS) constituted 91.8%, countries with records of one and two programs were 8.2, and 0% for countries without any participation (Fig. 1). Stepwise Approach to Surveillance pilot testing began in 2002, followed by a regional workshop series, which enabled many countries to conduct a first round of surveys between 2002 and 2003. This formed the basis upon which the study was built. Furthermore, the approach to STEP was dictated by the participants as enunciated.
|
|
A total of 56 countries participated in 17 regional or national workshops by 2005 (Fig. 2). Of these, 52 countries (14 in the WHO African Region, 1 in the WHO Region of the Americas, 11 in the WHO Eastern Mediterranean Region, 9 in the WHO South-East Asia Region, and 17 in the WHO Western Pacific Region) completed their data collection by the end of the year; this group includes the 6 countries that combined STEPS with their national risk-factor surveys. Of these, 28 were national surveys.
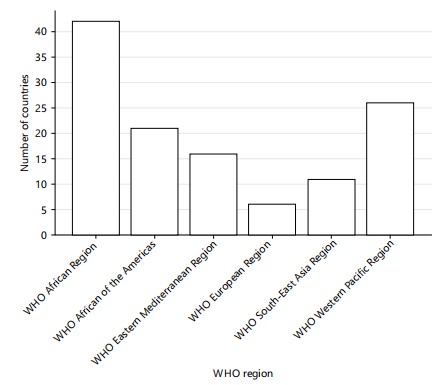
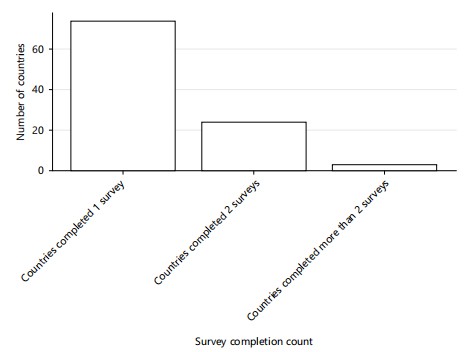
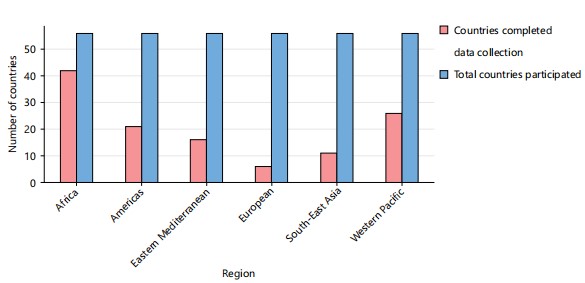
As of now, 129 countries and territories have signed up to participate in a total of 166 workshops, either with a national or regional focus (Fig. 3). Of these, data collection was completed in 122 countries, including 42 in the WHO African Region, 21 in the WHO Region of the Americas, 16 in the WHO Eastern Mediterranean Region, 6 in the WHO European Region, 11 in the WHO South-East Asia Region, and 26 in the WHO Western Pacific Region. Of these, 11 were consistent with STEPS guidelines. National surveys have been conducted in 93 countries in all. Forty-eight countries had multiple STEPS or STEPS-styled surveys, including 21 countries that transitioned from subnational to national surveys or had multiple subnational surveys. In addition, two STEPS or STEPS-aligned surveys have been conducted in 24 countries, and 3 countries continue to maintain a systematic and continuous process of multiple STEPS surveys25-27.
Of 122 countries that had finalized data collection at the time of this report, 10 countries provided data for only Steps 1 and 2 (questionnaires and physical measurements). However, 112 countries have done all three steps, including biochemical measurements.
Challenges: Figure 4 compares the number of countries that completed data collection under the WHO STEPS framework with the total participating countries across different WHO regions. The African Region showed the highest completion rate, while the European Region recorded the lowest. This disparity highlights regional challenges such as limited infrastructure, technical capacity, and logistical constraints, which affect the full implementation of the STEPS survey in some areas.
|
|
Although STEPS surveys have substantially scaled up in low and middle-income countries over the past decade, several challenges remain. Until the early 2000s, there was limited data available on NCDs in these regions. Nevertheless, STEPS surveys have experienced challenges in their extension, notably in rural and resource-constrained contexts. For most of these countries, collecting credible data on NCD risk factors was a major challenge, with the lack of adequate healthcare infrastructure, limited access to competent personnel, and logistical issues like transportation and patchy internet connectivity28,29. These challenges frequently jeopardize the quality and credibility of the data collected and add a layer of complexity to the incorporation of this data into national health systems. This finding is in line with a handful of researchers who posited on the similar challenges hampering efficient STEPS surveys across the globe30-32.
Adaptations: To meet these challenges, several adaptations should be made to the STEPS framework for it to be implemented successfully. Since trained healthcare personnel can only be found in limited
numbers in rural areas, many countries have recruited the help of community health workers (CHWs) to help with data collection, thus improving both the accuracy and reach of surveys. Others have integrated mobile health (mHealth) technologies to facilitate the process and deliver better-quality data collection33,34. These advances in technology have enabled more efficient surveillance and better integration of data into national health systems, even in the most remote regions. The efforts to adapt to logistical challenges also reinforced cultural sensitivity, which helped tailor survey methods and subsequent interpretation of data to local context and health beliefs. The position of these findings has also been reinforced by Hyder et al.33 and Song et al.34.
Outcomes: The STEPS survey implementation has yielded tremendous results. By 2025, over 129 countries had implemented the STEPS surveys, producing essential data on the NCD risk factors specific to their respective nations. This growth is a radical reversal of the early 2000s when hardly any data were available in low- and middle-income countries. There have already been almost 100 reports of survey results from individual countries in the form of country reports, journal articles, or summary data35-38.
These results have helped to inform national NCD policies and action plans. For instance, in four of the countries that conducted the STEPS survey, Benin, Cape Verde, Mauritania, and Togo, data from the STEPS were used to inform their national NCD strategies and exemplify the way that data-driven evidence is used to inform public health action39.
One of the biggest adaptations under the STEPS framework has been the introduction of “Data to Action” workshops that support countries in their efforts to accelerate NCD programming. The workshops have encouraged countries to collaborate and prioritize actions based on the latest and most trusted data by emphasizing addressing STEPS data needs nationally.
As observed in this study, the dissemination of findings from STEPS has supported new evidence-based interventions (EBIs) are integrated into clinical and community practice as posited by researchers35-38.
Global Impacti: The STEPS data has also fed into large global health initiatives. Several of the data derived from these surveys have been used in publications for the Global Burden of Disease Project, including reports on the prevalence of risk factors for different NCDs by global and regional estimates. Data is vital in understanding the global NCD landscape and providing guidance for policy decisions around the world, and it is growing in importance. Significantly, despite the evolution of the STEPS instruments over the years, the methods have also shown potential in resource-poor settings, supporting surveillance of NCDs and policy development.
As a whole, the implementation of STEPS surveys has resulted not only in the availability of strong and actionable data but also in demonstrating the adaptability of the STEPS methodology to cater to the specificities of countries in their response to NCDs. The STEPS has been successfully adapted to different local challenges, which created more inclusive, data-driven health policies and interventions worldwide, paving the way towards sustained advances in the battle against NCDs. The thinking of the authors of this study is in line with that of Piñeros et al.40.
Future directions: The need for comprehensive and comparable data on NCD risk factors at the national, regional, and global levels has become even more urgent following the global endorsement of the 9 voluntary targets for NCDs and the Global Monitoring Framework for NCD indicators. A multitude of risk factors tracked by STEPS surveys are incorporated into these frameworks, making WHO STEPS an indispensable instrument for tackling the impending global epidemic of Non-Communicable Diseases (NCDs). The STEPS surveys will provide the most needed data for 7 of the 9 global targets for NCDs: Tobacco use, harmful use of alcohol, physical inactivity, unhealthy diet, obesity, hypertension, and the prevention of heart attack and stroke. In addition, STEPS surveys support the tracking of other key indicators in the Global Monitoring Framework, including total cholesterol and cervical cancer screening.
Adopted by the world health assembly, the global action plan for the prevention and control of NCDs (2013) urges WHO Member States to routinely gather data on multiple behavioural and metabolic risk factors (e.g., harmful use of alcohol, tobacco use, physical inactivity, unhealthy diets, raised blood pressure, blood glucose and hyperlipidemia). This position agrees with WHO and UNESCO41-43.
Capacity building and sustainable NCD surveillance: A key future focus is strengthening capacity-building for STEPS technical assistance. This is essential to strengthen national surveillance capacity so that national health systems can monitor NCD risk factors over time. Greater country-level advocacy is required to ensure the inclusion of NCD-related data into national health information systems with robust, sustainable data systems that are also mainstay components of public health priorities and strategies. This stance is also agreed upon by Fouad et al.44.
The STEPS surveys are expected to be conducted every third to fifth year, but the recommended timeline is more challenging in low-resource settings. On the agenda going forward, extremely important is supporting countries in progressing from a baseline survey to implementing a regular cycle of risk-factor surveillance as part of their national NCD action plans. Similarly, countries with subnational surveys should be encouraged to take steps towards national-level implementation for more representative data that can guide policy change and resource distribution.
Adapting to new scientific and policy needs: It is necessary to hold periodic reviews of the questionnaire items and indicators used in STEPS surveys to ensure that the health science and policy needs keep pace with the advancement. Recent conversations have focused on more novel strategies, like incorporating wearables, to measure objectively patterns of physical activity and using haemoglobin A1c as an outcome for diabetes. With the advent of more reliable, cheaper, portable equipment, such innovations could be incorporated into population-based surveys such as STEPS, as recently highlighted. This aligns with Weir et al.45.
Expanding access to STEPS data: Access to the rich data stemming from STEPS surveys needs to be broadened urgently. At present, aggregate data are entered into the WHO Global InfoBase, although this system is dependent on voluntary reporting by countries. To facilitate the accessibility of STEPS data, there is a need to establish better channels that allow the data to be made available via one-stop platforms or portals (e.g., STEPS portal hosted by WHO), and from such portals, the data can be easily accessed to enhance evidence-based programming and policy decisions for NCDs. This perspective has also been advanced by Roberts et al.46.
Strengthening the link from data to action: Lastly, a central future priority is how to better link data and action at the country level. African countries have adopted pilot workshops, a promising approach in this area. The purpose of these workshops is to strengthen the link between STEPS data and actionable steps for policy development, target setting, and program implementation. Transforming evidence based on reliable, nationally representative NCD risk-factor data into tangible policy and programmatic action is invaluable for informing and guiding effective responses47-49.
The overall aim of STEPS is to improve the availability of data to help countries inform, monitor, and evaluate their NCD policies and programs. In the future, STEPS must continue to pursue this goal to make sure that NCD surveillance continues to improve the health of populations globally.
CONCLUSION
The global acceptance of the WHO STEPS approach for NCD risk factor surveillance as a scalable tool for non-communicable disease analysis in settings has been pivotal and paradigm-shifting. In the last decade, over 129 countries have adopted STEPS surveys, producing essential, country-specific data that directs national policies and solutions. The STEPS methodology has been a flexible approach adapted to low and middle-income countries facing unique challenges with resource constraints and logistical barriers to data collection. Even with significant progress made, enormous challenges remain, notably in rural regions with limited infrastructure and healthcare resources. To overcome these challenges, adaptations like the incorporation of mobile health technologies and the training of community health workers were essential to improving data quality and the sustainability of NCD surveillance initiatives. Going forward, the STPS surveys should continue to expand and be integrated into national health information systems to help achieve global NCD targets. In line with changing test and learning conditions, the STEPS framework will need to be reviewed and updated periodically to inform any new strategic directions on how best to use innovative technologies and scientific knowledge. STEPS will continue to be an integral part of enhancing global health outcomes by linking data collection to practical public health action areas, leading to reductions in the global burden of NCDs.
SIGNIFICANCE STATEMENT
This study identified the gaps associated with the WHO STEPS framework, which will significantly contribute to global NCD surveillance, enabling countries to formulate evidence-based health policies. The study will assist healthcare providers, health policy makers, and researchers the benefits of the STEP programs. Future success will depend on continued international support, inter-country data-sharing, and adaptive strategies to sustain and expand NCD prevention efforts globally.
REFERENCES
- Mudie, K., M.M.J. Tan, L. Kendall, J. Addo and I. dos-Santos-Silva et al., 2019. Non-communicable diseases in sub-Saharan Africa: A scoping review of large cohort studies. J. Global Health, 9.
- Sivanantham, P., J. Sahoo, S. Lakshminarayanan, Z. Bobby and S.S. Kar, 2021. Profile of risk factors for non-communicable diseases (NCDs) in a highly urbanized district of India: Findings from Puducherry district-wide STEPS survey, 2019-20. PLoS ONE, 16.
- Baatiema, L., O.A. Sanuade, L.N. Allen, S. Abimbola, C. Hategeka, K.A. Koram and M.E. Kruk, 2023. Health system adaptions to improve care for people living with non-communicable diseases during COVID-19 in low-middle income countries: A scoping review. J. Global Health, 13.
- Mundra, A., A. Kalantri, A. Jakasania, H. Sathe and A. Raut et al., 2023. Vitalizing community for health promotion against modifiable risk factors of noncommunicable diseases (V-CaN) in Rural Central India: Protocol for a hybrid type II implementation effectiveness trial. JMIR Res. Protoc., 12.
- van Bogaert, P., L. Peremans, D. van Heusden, M. Verspuy, V. Kureckova, Z. van de Cruys and E. Franck, 2017. Predictors of burnout, work engagement and nurse reported job outcomes and quality of care: A mixed method study. BMC Nurs., 16.
- Biswas, T., N. Townsend, R.D. Gupta, A. Ghosh, L.B. Rawal, K. Mørkrid and A. Mamun, 2023. Clustering of metabolic and behavioural risk factors for cardiovascular diseases among the adult population in South and Southeast Asia: Findings from WHO STEPS data. Lancet Reg. Health Southeast Asia, 12.
- Riley, L., R. Guthold, M. Cowan, S. Savin, L. Bhatti, T. Armstrong and R. Bonita, 2016. The World Health Organization STEPwise approach to noncommunicable disease risk-factor surveillance: Methods, challenges, and opportunities. Am. J. Public Health., 106: 74-78.
- Sung, M., J. He, Q. Zhou, Y. Chen, J.S. Ji, H. Chen and Z. Li, 2022. Using an integrated framework to investigate the facilitators and barriers of health information technology implementation in noncommunicable disease management: Systematic review. J. Med. Internet Res., 24.
- Alonge, O., S. Sonkarlay, W. Gwaikolo, C. Fahim, J.L. Cooper and D.H. Peters, 2019. Understanding the role of community resilience in addressing the Ebola virus disease epidemic in Liberia: A qualitative study (community resilience in Liberia). Global Health Action, 12.
- Hadian, M., M.R. Mozafari, E. Mazaheri and A. Jabbari, 2021. Challenges of the health system in preventing non-communicable diseases; systematized review. Int. J. Preventive Med., 12.
- Catley, D., T. Puoane, K. Goggin, L.P. Tsolekile and K. Resnicow et al., 2020. Adapting the diabetes prevention program for low- and middle-income countries: Preliminary implementation findings from lifestyle Africa. Transl. Behav. Med., 10: 46-54.
- Johns, B. and T. tan Torres, 2005. Costs of scaling up health interventions: A systematic review. Health Policy and Plann., 20: 1-13.
- Agoro, E.Y.S. and A. Alabere, 2025. Concentrations of selected metals and polycyclic aromatic hydrocarbons in fresh and fried Bayelsa Suya (Oryctes rhinoceros) sold in Bayelsa State, Nigeria. Asian Sci. Bull., 3: 32-38.
- Agoro, E.S. and F.U. Madu, 2024. Forensic significance of dried seminal and vaginal fluid, biochemical parameters in the corroboration of the occurrence of rape. Int. J. Health Res. Medico-Legal Pract., 10: 17-23.
- Agoro, E.Y.S., C.T. Adias and C.G. Ikimi, 2024. Use of Anopheles mosquito bloodmeal’s serology and haemoglobin genotypes in crime scene forensics. Asian J. Biol. Sci., 17: 574-581.
- Agoro, E.Y.S. and C.G. Ikimi, 2022. Translocation capacity of some heavy metals in aquatic food chain of crude oil impacted community of Imiringi in Bayelsa State, Nigeria. Toxicol. Res. Appl., 6.
- Agoro, E.Y.S. and J.T. Johnson, 2022. Translocation concept of heavy metals in plantain consumption chain of crude oil impacted community in Bayelsa State Nigeria. J. Ind. Pollut. Control, 38.
- Aerts, N., S. Anthierens, P. van Bogaert, L. Peremans and H. Bastiaens, 2022. Prevention of cardiovascular diseases in community settings and primary health care: A pre-implementation contextual analysis using the consolidated framework for implementation research. Int. J. Environ. Res. Public Health, 19.
- Leon, N. and H. Xu, 2023. Implementation considerations for non-communicable disease-related integration in primary health care: A rapid review of qualitative evidence. BMC Health Serv. Res., 23.
- Kazmi, T., M.L.F. Nagi, S. Razzaq, S. Hussnain, N. Shahid and U. Athar, 2022. Burden of noncommunicable diseases in Pakistan. East. Mediterr. Health J., 28: 798-804.
- Al-Mawali, A., S.K. Jayapal, M. Morsi, W. Al-Shekaili and A.D. Pinto et al., 2021. Prevalence of risk factors of non-communicable diseases in the Sultanate of Oman: STEPS survey 2017. PLoS ONE, 16.
- Saeed, K., M.H. Rasooly and M. Nejaby, 2020. Profile of risk factors for noncommunicable diseases in major cities of Afghanistan: WHO STEPwise approach. East. Mediterr. Health J., 26: 388-399.
- Bista, B., M. Dhimal, S. Bhattarai, T. Neupane and Y.Y. Xu et al., 2021. Prevalence of non-communicable diseases risk factors and their determinants: Results from STEPS survey 2019, Nepal. PLoS ONE, 16.
- Juma, P.A., C. Mapa-Tassou, S.F. Mohamed, B.L.M. Mwagomba and C. Ndinda et al., 2018. Multi-sectoral action in non-communicable disease prevention policy development in five African countries. BMC Public Health, 18.
- Tesema, A.G., S. Abimbola, A. Mulugeta, W.S. Ajisegiri, P. Narasimhan, R. Joshi and D. Peiris, 2021. Health system capacity and readiness for delivery of integrated non-communicable disease services in primary health care: A qualitative analysis of the Ethiopian experience. PLOS Global Public Health, 1.
- Budreviciute, A., S. Damiati, D.K. Sabir, K. Onder and P. Schuller-Goetzburg et al., 2020. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front. Public Health, 8.
- Okop, K., P. Delobelle, E.V. Lambert, H. Getachew and R. Howe et al., 2023. Implementing and evaluating community health worker-led cardiovascular disease risk screening intervention in Sub-Saharan Africa communities: A participatory implementation research protocol. Int. J. Environ. Res. Public Health., 20.
- Adeyemi, O., M. van den Bold, N. Nisbett and N. Covic, 2022. Changes in Nigeria’s enabling environment for nutrition from 2008 to 2019 and challenges for reducing malnutrition. Food Sec., 15: 343-361.
- Ahmadi, M., F.K. Nezhad and H. Parsipour, 2025. Mid-term program in urban peripheral: A case study of Kalateh Yavari village in Bojnord country. Village Space Sustainable Dev.
- Al Kibria, G.M., S. Ahmed, I.A. Khan, J.A. Fernández-Niño and A. Vecino-Ortiz et al., 2023. Developing digital tools for health surveys in low- and middle-income countries: Comparing findings of two mobile phone surveys with a nationally representative in-person survey in Bangladesh. PLOS Global Public Health, 3.
- Kilpeläinen, K., P. Koponen, H. Tolonen, S. Koskinen, K. Borodulin and M. Gissler, 2019. From monitoring to action: Utilising health survey data in national policy development and implementation in Finland. Arch. Public Health., 77.
- Bastawrous, A. and M.J. Armstrong, 2013. Mobile health use in low- and high-income countries: An overview of the peer-reviewed literature. J. R. Soc. Med., 106: 130-142.
- Hyder, A.A., A.C. Wosu, D.G. Gibson, A.B. Labrique, J. Ali and G.W. Pariyo, 2017. Noncommunicable disease risk factors and mobile phones: A proposed research agenda. J. Med. Internet Res., 19.
- Song, Y., R. Phadnis, J. Favaloro, J. Lee and C.Q. Lau et al., 2020. Using mobile phone data collection tool, surveda, for noncommunicable disease surveillance in five low- and middle-income countries. Online J. Public Health Inf., 12.
- Carvalho, M.L., S. Honeycutt, C. Escoffery, K. Glanz, D. Sabbs and M.C. Kegler, 2013. Balancing fidelity and adaptation: Implementing evidence-based chronic disease prevention programs. J. Public Health Manage. Pract., 19: 348-356.
- Castro, G.F., M. Barrera and C.R. Martinez, 2004. The cultural adaptation of prevention interventions: Resolving tensions between fidelity and fit. Prev. Sci., 5: 41-45.
- Galbraith, J.S., B. Stanton, B. Boekeloo, W. King and S. Desmond et al., 2008. Exploring implementation and fidelity of evidence-based behavioral interventions for HIV prevention: Lessons learned from the focus on kids diffusion case study. Health Educ. Behav., 36: 532-549.
- Stirman, S.W., J. Kimberly, N. Cook, A. Calloway, F. Castro and M. Charns, 2012. The sustainability of new programs and innovations: A review of the empirical literature and recommendations for future research. Implementation Sci., 7.
- Escoffery, C., E. Lebow-Skelley, H. Udelson, E.A. Böing, R. Wood, M.E. Fernandez and P.D. Mullen, 2019. A scoping study of frameworks for adapting public health evidence-based interventions. Transl. Behav. Med., 9: 1-10.
- Piñeros, M., A. Znaor, L. Mery and F. Bray, 2017. A global cancer surveillance framework within noncommunicable disease surveillance: Making the case for population-based cancer registries. Epidemiologic Rev., 39: 161-169.
- WHO, 2018. Global Action Plan on Physical Activity 2018-2030: More Active People for a Healthier World. World Health Organization, Geneva, Switzerland, ISBN-9789241514187, Pages: 101.
- WHO., 2010. Global Recommendations on Physical Activity for Health. World Health Organization, Geneva, Switzerland, ISBN-13: 9789241599979, Pages: 58.
- Bartholomew, J.B. and E.M. Jowers, 2011. Physically active academic lessons in elementary children. Preventive Med., 52: S51-S54.
- Fouad, H., N. Abdel Latif, R.A. Ingram and A. Hammerich, 2018. Scaling up prevention and control of noncommunicable diseases in the WHO Eastern Mediterranean Region. East. Mediterr. Health J., 24: 52-62.
- Weir, K.R., N.J. Ailabouni, C.R. Schneider, S.N. Hilmer and E. Reeve, 2022. Considerations for systematic reviews of quantitative surveys: Learnings from a systematic review of the patients’ attitudes towards deprescribing questionnaire. Res. Social Administrative Pharm., 18: 2345-2349.
- Roberts, J., C. Onuegbu, B. Harris, C. Clark and F. Griffiths et al., 2025. Comparing in-person and remote qualitative data collection methods for data quality and inclusion: A scoping review. Int. J. Qual. Methods., 24.
- Lemma, S., A. Janson, L.Å. Persson, D. Wickremasinghe and C. Källestål, 2020. Improving quality and use of routine health information system data in low- and middle-income countries: A scoping review. PLoS ONE, 15.
- Sharma, A., S.K. Rana, S. Prinja and R. Kumar, 2016. Quality of health management information system for maternal & child health care in Haryana State, India. PLoS ONE, 11.
- O'Hagan, R., M.A. Marx, K.E. Finnegan, P. Naphini and K. Ng'ambi et al., 2017. National assessment of data quality and associated systems-level factors in Malawi. Global Health Sci. Pract., 5: 367-381.
How to Cite this paper?
APA-7 Style
Nathan,
A.O., Onyeuche,
O.A. (2025). Implementation of the WHO STEPS Approach for NCD Risk Factor Surveillance in Rural Communities: Challenges, Adaptations, and Outcomes. Trends in Medical Research, 20(1), 8-20. https://doi.org/10.3923/tmr.2025.08.20
ACS Style
Nathan,
A.O.; Onyeuche,
O.A. Implementation of the WHO STEPS Approach for NCD Risk Factor Surveillance in Rural Communities: Challenges, Adaptations, and Outcomes. Trends Med. Res 2025, 20, 8-20. https://doi.org/10.3923/tmr.2025.08.20
AMA Style
Nathan
AO, Onyeuche
OA. Implementation of the WHO STEPS Approach for NCD Risk Factor Surveillance in Rural Communities: Challenges, Adaptations, and Outcomes. Trends in Medical Research. 2025; 20(1): 8-20. https://doi.org/10.3923/tmr.2025.08.20
Chicago/Turabian Style
Nathan, Agoro,, Oviemova, and Osom Alexanda Lott Onyeuche.
2025. "Implementation of the WHO STEPS Approach for NCD Risk Factor Surveillance in Rural Communities: Challenges, Adaptations, and Outcomes" Trends in Medical Research 20, no. 1: 8-20. https://doi.org/10.3923/tmr.2025.08.20

This work is licensed under a Creative Commons Attribution 4.0 International License.