Assessment of Filling of Relevant Information on the Laboratory Request Forms
-
B.O. Adegoke
Department of Chemical Pathology, Ekiti State University, Nigeria
A.S. Atiba

Department of Chemical Pathology, Ekiti State University, Nigeria
B.O. AdegokeDepartment of Pharmacology and Therapeutics, Ekiti State University, Nigeria
T.A. Niran-AtibaDepartment of Biomedical Sciences, Ladoke Akintola University of Technology, Ogbomoso, Nigeria
| Received 17 Nov, 2023 |
Accepted 26 Feb, 2024 |
Published 06 Mar, 2024 |
Background and Objective: It has been observed in the recent past, that the importance of preventing pre-analytical errors was reported to cause as high as 67% of errors observed in laboratory results. The errors in this phase of analysis are still unresolved even with the advent of autoanalyzers. The objective of this study was to analyze the contribution of inadequate filling of request forms to pre-analytical errors. Materials and Methods: The research was a cross-sectional study that was carried out on in- and outpatient request forms received from various sections of the hospital over a period of three months. A protocol table was created to capture variables. The analysis included all request forms obtained in each of the four laboratories as well as those obtained from other hospitals in the environment. Data were analyzed by the use of SPSS version 23. Variables were summarised by mean and frequency tables. Results: The age of the patient was missing from 14.6% of the forms. The gender of the patients was missing in 1.3% of cases. The time of sample collection was specified in 105 (10.5%) request forms but was left blank in 895 (89.5%) forms. In 303 (30.3%) of the forms, the date of sample collection was missing. In 989 (98.9%) of the forms, the current medication history of the patients was not provided. The clinical summary was provided in 856 (85.6%) forms while it was not indicated in 126 (12.6%) of the forms. Conclusion: Only the patients’ names and the investigations required were filled in all the forms. All other parameters on the laboratory request forms were not fully completed.
| Copyright © 2024 Adegoke et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
In the past, clinical history and physical examination of patients were the major diagnostic tools in the assessment of patients1. Recently, consideration of laboratory results in the assessment of patients is increasing daily. In other words, the roles of clinical laboratories in the healthcare delivery system cannot be overemphasized2. The laboratory is a significant component of the hospital set-up especially in the areas of disease diagnosis and the eventual treatment of patients. The prompt sample analysis and result interpretation in the laboratory guide the doctor in decision-making about the treatment3. Prevention of errors on the laboratory parameters has been historically determined by the accuracy of the analytical phase of the analysis following the development of high-quality analytical techniques, especially those incorporated in auto analyzers. Prevention of pre-analytical errors is becoming more important than analytical errors in the laboratory testing procedures4.
Thirty-one to sixty-seven percent of laboratory errors occur in the pre-analytical phase and one of the common ones is the improper filling of laboratory test request forms5. To reduce pre-analytical errors to an acceptable level, the request forms from various sections of the hospital must be correctly and adequately filled. It allows physicians in the laboratory, among other things to relate results with the clinical summary of the patient which may be a pointer to the possibility of errors that may be as a result of either faulty laboratory analysis or in the working clinical diagnosis as indicated by the requesting physician6.
Total quality control management plays a major role in providing quality and reliable laboratory results for the subsequent provision of adequate care for the patients7. In Africa, especially in resource-poor settings where laboratory information systems are still not available in the majority of the hospitals, manual processing of request forms is still a common practice which is prone to errors that may result from illegible handwriting. The use of nonconventional abbreviations and incomplete entry of necessary data on the request form are likely sources of errors as well8.
Request forms are designed to obtain vital bio-data and clinical information from patients whose samples are being analysed3. The incompleteness of the request form generates a lot of clinical issues, one of which is difficulty in interpreting the results and consequently poor management of patients9. A greater percentage of these human errors in the pre-analytical phase have been reported in different centers including some centers in Nigeria. This has never been studied in our center and the findings of this will go a long way in knowing which area to advise clinicians on for better healthcare delivery services. Hence this study was aimed at evaluating the pattern of filling of request forms in the four laboratory units of the Ekiti State University Teaching Hospital, Ado-Ekiti.
MATERIALS AND METHODS
Study area: The research was carried out on in and out-patient request forms which were filled by the physicians and sent to the laboratory receptions of the Ekiti State University Teaching Hospital (EKSUTH) Ado-Ekiti between July and October 2023.
Sample size: Out of 1,367 requests that were received during the study period as observed from the register, only 1000 request forms were included in the analysis. The reasons for excluding those that were not used were: Samples were not seen with some request forms, some request forms were not seen despite having them received in the laboratory reception according to the register and some results (emergency parameters) were already released to the patients before our research team could get to assess them.
Study design: The study was a cross-section study that was carried out within three months in the Departments of Chemical Pathology, Haematology, Medical Microbiology and Anatomic Pathology. The following variables were considered: Patient’s full name, age, date of birth, gender (sex), hospital number, ward/clinic, nature of the specimen, consultant’s name, resident doctor’s signature, clinical summary, time of sample collection and test requested for. A protocol table was designed to record variables as mentioned. The results were collated according to the request from each clinical department and the number recorded per day was taken into consideration as well.
All request forms received in each of the four departments in the laboratory and those received from other hospitals in the community were included in the study. Request forms without the attached sample were excluded from the study.
Ethical consideration: The conduct of this study was permitted by the Research and Ethical Committee of the Ekiti State University Teaching Hospital, Ado-Ekiti with protocol number EKSUTH/A67/2023/06/009.
Statistical analysis: Data were collated and summarised by mean and frequency of continuous variables with the aid of SPSS version 23. The data were also displayed using a bar chart.
RESULTS
As observed in Table 1, a total of 1000 request forms were reviewed from the four units of the laboratory within the study period. Chemical pathology has the highest requests (41.2%), followed by Haematology requests (27.8%), Medical Microbiology requests (18.3%) and Anatomic Pathology requests (12.7%). It was observed that certain patients’ information and other data were not uniformly required by all the units in the laboratory.
In all the forms the name and the requested tests were present. In about eighty-five percent of cases (85.4%), the ages of the patient were filled, however, 14.6% of the request forms did not contain the ages of the patients. Also, for the gender of patients, 987 (98.7%) forms did have the gender of the patient while 13 (1.3%) did not contain the gender of the patients. The time of sample collection was filled in 105 (10.5%) but absent in 895 (89.5%) of the request forms received. The date of sample collection was present in 697 (69.7%) and absent in 303 (30.3%) request forms received. The current medication history of patients was indicated in 11 (1.1%) filled request forms and 989 (98.9%) did not indicate it. Clinical summary was stated in 856(85.6%) while 126 (12.6%) did not contain such information. The abbreviation was used in some request forms which are not standard. The name of the consultant-in-charge was omitted in 255 (25.5%) of the request forms. The doctor’s signature was present in 779 (77.9%) of the request form received. Ethnicity was omitted in 900 (90%) request forms. The hospital number was present in 691 (69.1%) of the forms received. Nationality was only present in 69 (6.9%) and phone numbers were present in 101 request forms. Also, the home address was written in 42 request forms, email address of the patient was omitted in 995 (99.5%) of cases.
DISCUSSION
Pre-analytical errors can negatively impact the quality of laboratory results with associated adverse consequences on diagnosis and eventual treatment of patients. Request forms are a medium of communication between physicians and laboratories where the tests are carried out, especially in settings where electrically generated request forms are not available. One can say that the advent of computers and their usage in clinical laboratories must have limited the occurrence of analytical errors. However, because, largely pre-analytical activities are still done manually, errors still occur in this phase of analysis. The pre-analytical phase is without the full control of laboratory staff. For instance, the filling of request forms is done by physicians in the clinics and the wards. Clinicians and other groups of hospital staff are majorly responsible for the collection of specimens and transportation of the same to the concerned laboratory. In this study, 1000 laboratory request forms were evaluated to examine the pattern in which the request forms are filled.
The name of the patient and the investigation requested were filled in all the request forms. We found out from other studies that the pattern was not too different, although none of these other studies recorded a 100% rate as we observed in our study10-12. According to a cross-sectional descriptive study conducted in Pakistan, Rawalpindi; out of a total of 1000 forms studied, none was fully filled13. The clinical summary was present only in 13% of the forms. This is contrary to this study, about 85.6% of the request forms studied have clinical summaries (Table 2). This finding was similar to those of Nutt et al.14. The clinical summary provides a guide as to whether a patient is newly diagnosed or patient on a regular visit to the hospital, this helps to determine the quality of treatment based on the laboratory result generated and all these cannot be decided on an incompletely filled request form. What is of note in our study is that some request forms came with some unconventional abbreviations which is capable of making result interpretation difficult.
| Table 1: | Request forms received in various laboratories | |||
| Laboratory | Frequency |
Percentage |
| Haematology | 278 |
27.8 |
| Chemical pathology | 412 |
41.2 |
| Medical microbiology | 183 |
18.3 |
| Anatomic pathology | 127 |
12.7 |
| Total | 1000 |
100 |
| Table 2: | Variables on request forms (directly influence outcome of the results) | |||
| Variable | Frequency |
Percentage |
| Age | ||
| Present | 854 |
85.4 |
| Absent | 146 |
14.6 |
| Total | 1000 |
100 |
| Gender | ||
| Present | 987 |
98.7 |
| Absent | 13 |
1.3 |
| Total | 1000 |
100 |
| Time of sample collection | ||
| Present | 105 |
10.5 |
| Absent | 895 |
89.5 |
| Total | 1000 |
100 |
| Medication | ||
| Present | 11 |
1.1 |
| Absent | 989 |
98.9 |
| Total | 1000 |
100 |
| Clinical summary | ||
| Present | 856 |
85.6 |
| Absent | 126 |
12.6 |
| Abbreviation | 18 |
1.8 |
| Total | 1000 |
100 |
| Nature of the specimen | ||
| Present | 894 |
89.4 |
| Absent | 106 |
10.6 |
| Total | 1000 |
100 |
As it was also shown in Table 2, the time of sample collection was only stated in 10.5% of the forms received over the study period. This is a common occurrence in previous studies10-15. The importance of indicating the time of sample collection cannot be overvalued. Some biochemical parameters such as bicarbonate are reduced in concentration with a delay in sample analysis3. Knowing the time of sample collection makes the analyst suspect possible pre-analytical errors which may be an indication to reject the sample for the analysis for fear of not getting accurate results. Another notable omission in the request form as observed from our study is the habit of requesting doctors not to indicate what medication the patient is being given. Medication history was only present in 1.1% of the forms studied. This is important because of the known effects of some medications on some biochemical parameters15. However, one of the reasons that may have accounted for this low indication of medication history may be because some patients who were coming newly to the hospital were included. This set of patients had not been placed on any medication except drugs that are self-prescribed which may not be volunteered to the attending physician.
This study also observed that important information such as hospital numbers which are crucial for patient identification, especially in database entry and for patient confidentiality were missing in a considerable number of request forms. Furthermore, patients’ ages were either absent or inappropriately filled in 146 (14.6%) forms that were reviewed. This appears to be low compared to the study done by Alagoa and Udoye11. The importance of filling the age of the patient on the laboratory request form cannot be over-recognized. Some laboratory investigations are age-dependent, especially age-related reference intervals. Many clinical conditions are common in certain age groups.
| Table 3: | Variables on request forms (indirectly influence outcome of the results) | |||
| Variable | Frequency |
Percentage |
| Date | ||
| Present | 697 |
69.7 |
| Absent | 303 |
30.3 |
| Total | 1000 |
100 |
| Name of consultant in charge | ||
| Present | 745 |
74.5 |
| Absent | 255 |
25.5 |
| Total | 1000 |
100 |
| Doctor’s signature | ||
| Present | 779 |
77.9 |
| Absent | 221 |
22.1 |
| Total | 1000 |
100 |
| Ethnicity | ||
| Present | 100 |
10 |
| Absent | 900 |
90 |
| Total | 1000 |
100 |
| Hospital number | ||
| Present | 691 |
69.1 |
| Absent | 309 |
30.9 |
| Total | 1000 |
100 |
| Nationality | ||
| Present | 69 |
6.9 |
| Absent | 931 |
93.1 |
| Total | 1000 |
100 |
| Phone number | ||
| Present | 101 |
10.1 |
| Absent | 899 |
89.9 |
| Total | 1000 |
100 |
| Home address | ||
| Present | 42 |
4.2 |
| Absent | 958 |
95.8 |
| Total | 1000 |
100 |
| Email address of the requesting doctor | ||
| Present | 5 |
0.5 |
| Absent | 995 |
99.5 |
| Total | 1000 |
100 |
As presented in Table 3, the majority of the request forms studied were requested by a physician as indicated by writing the name of the consultant-in-charge of the patients and signed by the junior doctor on the ground. This was in agreement with a study in which 62% of the expensive specialized investigations were requested by consultant specialists while 38% were ordered by resident doctors and general practitioners but the percentage of the avoidable expensive tests that were ordered by the general practitioners and resident doctors was significantly higher than that of the specialists13. However, the current study observed that 25.5% of forms did not have the name of the consultant in-charge, which is higher compared to what was noted in Alagoa and Udoye11. The signature of the requesting doctor was not filled in 22.1% as shown from this study. This was similar to the findings presented in the study by Adegoke et al15.
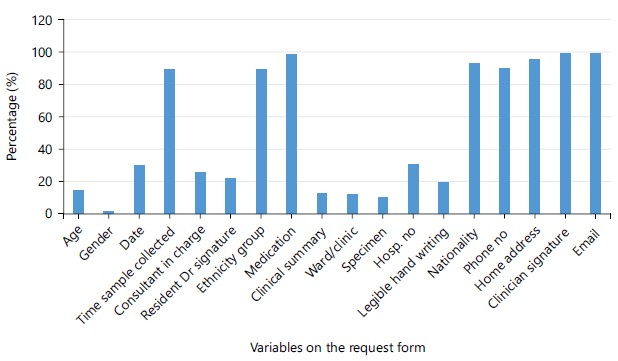
As shown in Fig. 1, the pattern of filling out request forms for important variables was summarised. This pattern was similar to findings from previous studies11,15. In another study from South Africa, a total of 2550 request forms were studied. Drug usage by patients (89.6%) and mobile contacts of requesting physicians (61.2%) were the most incompletely filled parameters. In 19.1% of request forms, there was no clinical diagnosis filled, even in some with clinical working diagnoses they were presented in an unconventional abbreviation in 37.3% of the request forms. This accounted for 35.5% of diagnoses that were not recorded at the reception unit of the laboratory because the staff in this unit were not able to understand these unconventional abbreviations. Insufficient information about the ward where these forms were being brought in was found in 4.9% of the forms examined14. In another separate study, the impact of 151 request forms that were collected over a period of eight months, with incomplete ward location information, critical results could not be communicated by telephone to clinicians in 19.9% of cases14.
|
In Lagos, Nigeria, a different study evaluated the completeness of 527 laboratory request forms for pre- and post-education on how the form should be filled. The results indicated that the name was completed 100% of the time in both pre-and post-education evaluation, the age was completed 78% of the times in pre- and 97% of the times in post-education evaluation and the sex was completed in 95% of the times in pre- and 99% of the times in post-education evaluation. The hospital number was filled in only 42% of the times in pre- and 67% of the times in post-education, the ward was filled in 81% of the times and 85% of the times in pre- and post-education respectively and the clinical diagnosis was filled in 82% of the times in pre-education and 99% of the times in post-education evaluation16. This demonstrated the necessity for continuous education to ensure that doctors understand the significance of accurately filling out request forms and how doing so helps to reduce pre-analytical errors. This could be the reason many studies are being conducted in different centers in this field. Those studies like ours aim to provide a scientific foundation for counseling doctors who fill out request forms.
Another research carried out in Ile-Ife, Nigeria, is comparable to ours when it comes to explaining the variables in Fig. 1, some of which have already been discussed previously15. Two thousand, one hundred and fifteen (2115) request forms in all were evaluated. The patient's name, which matches what we saw in our study, was the sole well-documented parameter. In 10.3 and 36.5% of the forms, the specimen collection time and date were noted, respectively. About eighty-six percent (86.4%) of the population had their dates of birth documented. It is important to note that the request forms studied in this current research did not have a date of birth section, which we believe is an omission that has to be corrected before printing more forms in the future. When one knows a patient's date of birth, the age can be computed accurately and compared with the patient's stated age. In 93.2% of cases, the working diagnosis was noted. Regarding medication history, there was no information available for every patient. Only 92.2% of forms have a properly written working diagnosis. The consultant in charge was mentioned in 96.6% of cases15.
It was observed in this study that the rate of omission of these variables is not as much as in the previous studies15. However, there is still a need to educate our clinicians about the proper filling of the laboratory request forms. This can be done by joint regular meetings between the laboratory physicians and the clinicians, where the issues of patient management are discussed.
CONCLUSION
This study observed that only the patients’ names and the investigations required were filled in all the forms. All other parameters on the laboratory request forms were not fully completed. A greater percentage of physicians still didn’t fill in the time of sample collection and the current medication history of the patient on the forms. Results recommended that all clinicians make efforts to properly fill laboratory request forms for adequate and effective result interpretation for the eventual benefit of the patients. Training of laboratory receptionists to identify incomplete filled forms is highly recommended. These are sets of errors the advent of electronic medical records (EMR) cannot adequately solve.
SIGNIFICANCE STATEMENT
The advent of computers and their applications in clinical laboratories has resolved some analytical errors. However, this has not greatly helped in solving pre-analytical errors because the majority of the processes involved are still performed manually, especially in a low-resource setting like ours. Inadequate filling of request forms may contribute to these pre-analytical errors. This study, therefore, looked into the pattern of filling out request forms that are received in the laboratories and it was observed that clinicians do not always properly complete laboratory investigation forms. Critical information is not provided. And this can greatly affect patients’ result interpretations and subsequently, patients’ management. Regular training of health workers in this regard is recommended.
REFERENCES
- Hampton, J.R., M.J. Harrison, J.R. Mitchell, J.S. Prichard and C. Seymour, 1975. Relative contributions of history-taking, physical examination, and laboratory investigation to diagnosis and management of medical outpatients. Br. Med. J., 2: 486-489.
- Oyelekan, A.A., O.T. Ojo, O.O. Olawale, O.O. Adeleye, O.A. Sogebi, O.A. Osinupebi and P.O. Olatunji, 2018. Pattern of completion of laboratory request forms in a tertiary health facility. Ann. Health Res., 4: 155-161.
- Olumide, O.B., A.O. Joel, M.E. Paul, A.C. Nedolisa and S.K. Oyero et al., 2019. Assessment of patients' medical laboratory request forms for compliance in Jos University Teaching Hospital, Jos-Nigeria. Am. J. Biomed. Sci. Res., 6: 334-339.
- Bonini, P., M. Plebani, F. Ceriotti and F. Rubboli, 2002. Errors in laboratory medicine. Clin. Chem., 48: 691-698.
- Olayemi, E. and R. Asiamah-Broni, 2011. Evaluation of request forms submitted to the haematology laboratory in a Ghanaian tertiary hospital. Pan Afr. Med. J., 8.
- Adamu, S., A. Mohammed, J.M. El-Bashir, J.D. Abubakar and D.S. Mshelia, 2018. Incomplete patient data on chemical pathology laboratory forms in a Tertiary Hospital in Nigeria. Ann. Trop. Pathol., 9: 47-49.
- Barak, M. and R. Jaschek, 2014. A new and effective way for preventing pre-analytical laboratory errors. Clin. Chem. Lab. Med., 52: e5-e8.
- Schroeder, L.F. and T. Amukele, 2014. Medical laboratories in Sub-Saharan Africa that meet international quality standards. Am. J. Clin. Pathol., 141: 791-795.
- Imoh, L.C., C.P. Onyenekwu, K.O. Inaku , A.O. Abu, C.D. Tagbo, I.Y. Mohammed and M.A. Kuti, 2021. Multicenter survey of physicians' perception of interpretative commenting and reflective testing in Nigeria. J. Int. Fed. Clin. Chem. Lab. Med., 32: 85-97.
- Burton, J.L. and T.J. Stephenson, 2001. Are clinicians failing to supply adequate information when requesting a histopathological investigation? J. Clin. Pathol., 54: 806-808.
- Alagoa, P.J. and E.P. Udoye, 2015. Laboratory request forms-How well do doctors fill them? A look at the practice at the Niger Delta University Teaching Hospital, Okolobiri, Bayelsa State, Nigeria. Niger. Health J., 15: 14-17.
- Chhillar, N., S. Khurana, R. Agarwal and N.K. Singh, 2011. Effect of pre-analytical errors on quality of laboratory medicine at a neuropsychiatry institute in North India. Ind. J. Clin. Biochem., 26: 46-49.
- Malik, M.F., D.A. Khan, W.M. Ansari and F.A. Khan, 2013. Injudicious use of laboratory facilities in tertiary care hospitals at Rawalpindi, Pakistan: A cross-sectional descriptive study. BMC Health Serv. Res., 13.
- Nutt, L., A.E. Zemlin and R.T. Erasmus, 2008. Incomplete laboratory request forms: The extent and impact on critical results at a tertiary hospital in South Africa. Ann. Clin. Biochem., 45: 463-466.
- Adegoke, O.A., A.A. Idowu and O.A. Jeje, 2011. Incomplete laboratory request forms as a contributory factor to preanalytical errors in a Nigerian teaching hospital. Afr. J. Biochem. Res., 5: 82-85.
- Osegbe, I.D., O. Afolabi and C.P. Onyenekwu, 2016. The effectiveness of clinician education on the adequate completion of laboratory test request forms at a tertiary hospital. Ann. Med. Health Sci. Res., 6: 90-94.
How to Cite this paper?
APA-7 Style
Adegoke,
B.O., Atiba,
A.S., Adegoke,
B.O., Niran-Atiba,
T.A. (2024). Assessment of Filling of Relevant Information on the Laboratory Request Forms. Trends in Medical Research, 19(1), 57-64. https://doi.org/10.3923/tmr.2024.57.64
ACS Style
Adegoke,
B.O.; Atiba,
A.S.; Adegoke,
B.O.; Niran-Atiba,
T.A. Assessment of Filling of Relevant Information on the Laboratory Request Forms. Trends Med. Res 2024, 19, 57-64. https://doi.org/10.3923/tmr.2024.57.64
AMA Style
Adegoke
BO, Atiba
AS, Adegoke
BO, Niran-Atiba
TA. Assessment of Filling of Relevant Information on the Laboratory Request Forms. Trends in Medical Research. 2024; 19(1): 57-64. https://doi.org/10.3923/tmr.2024.57.64
Chicago/Turabian Style
Adegoke, B., O., A. S. Atiba, B. O. Adegoke, and T. A. Niran-Atiba.
2024. "Assessment of Filling of Relevant Information on the Laboratory Request Forms" Trends in Medical Research 19, no. 1: 57-64. https://doi.org/10.3923/tmr.2024.57.64

This work is licensed under a Creative Commons Attribution 4.0 International License.