Glycemic Control in Diabetic Patients During COVID-19 Pandemic, A Study from North Al-Batinah, Oman
-
Firdous Jahan

Department of Family Medicine College of Medicine and Health Sciences(COMHS), National University Science and Technology, Sohar, Oman
Sanam AnwarNational University Science and Technology, Sohar, Oman
Ibrahim Fadhil Al ShibliDepartment of Primary Health Care Supportive Services, Directorate General of Health Services of North Al Batinah Governorate, Ministry of Health, Oman
Buthaina Khalifa Al SaadiFalaj Al-Qabail Health Centre, Ministry of Health, Oman
Asil Asim Al GhaithiGeneral Foundation Program, Oman Medical Specialty Board
Iman Hamdan Al MamariGeneral Foundation Program, Oman Medical Specialty Board
| Received 15 Aug, 2023 |
Accepted 30 Nov, 2023 |
Published 02 Dec, 2023 |
Background and Objective: The prevalence of diabetes is persistently rising. Diabetics are prone to infections that can affect glycemic control. Recent COVID-19 pandemic coupled with the increased global burden of diabetes. The current study was done to find the glycemic control of diabetic patients during COVID-19 pandemic. Materials and Methods: A retrospective cross-sectional observational study was conducted wherein the clinical and laboratory parameters were extracted from the computerized databases using a predesigned questionnaire. The HbA1C lab values were checked for the registered participants from 2018 to 2021. The chi-square test was used to compare the frequency of uncontrolled and controlled diabetes covariates. Paired t-test was used to compare mean HbA1c values. Results: A total of 314 diabetic patients were studied, 66.66% were females, 58.6% were more than 60 years and 33.1% were 45-60 years. A statistically significant difference (p<0.05) was found between liver disease patients in uncontrolled (25%) and controlled diabetes (64.4%). The study showed that control of diabetes worsened with the advent of COVID. Uncontrolled diabetes was 63.4% in 2018 before COVID-19 started and subsequently increased from 2019 (64.6%) to 2020 (69.7%) to 2021 (70.4%). There was a significant mean difference in HbA1c readings between 2018-2020 (p<0.05); 2019-2020 (p<0.01) and 2019-2021 (p<0.01). Conclusion: The current study showed that during COVID the control of diabetes declined as evidenced by HbA1c values of 7.8 pre-COVID to 8.1 post-COVID suggesting that during COVID, patients did not get optimal care and could not visit hospitals often for advice which led to uncontrolled diabetes. This suggested COVID-19 affected HbA1c status supporting the hypothesis towards uncontrolled diabetes.
| Copyright © 2023 Jahan et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
The prevalence of diabetes in the year 2010 was estimated to be 6.4% worldwide. Between 2010 and 2030, 73% increase in adult diabetes numbers in developing countries, compared to a 20% increase in developed countries1. The COVID-19 pandemic has changed the way that chronic health care is delivered. The need for physical distancing and the burden of infectious disease due to COVID-19 in primary healthcare inhibited a lot of normal healthcare processes2,3. The COVID-19 guidance to reduce risk, diabetic patients’ control. Healthcare providers are involved in diabetic care ensuring good glycemic control, continuous access to essential diabetes medications, appropriate diabetes education and care for patients4,5. Patients are avoiding routine appointments out of fear of infection from those also attending the clinic and perhaps are recognized to be at high risk of infection6. Moreover, the patients who are responsible for self-care at home now more concerned as they cannot freely go to primary care. They are advised to follow general guidance on risk reduction, including social distancing and hand washing, more frequent blood glucose monitoring and to take influenza and pneumonia vaccinations7,8. Obesity, heart or kidney disease require special care to stabilize their cardiac/renal status. Also need to follow their routine including checking their feet daily, keeping a healthy diet and keeping them active9. In Oman, the crude prevalence of diabetes among middle-aged adults was 16.1%. 5 32% of patients admitted for COVID-19 were known to have diabetes.
A study from Oman revealed that DM services were accessible in primary care during COVID-19 pandemic as a majority of patients maintained follow-up in 2020, despite the disruption of comprehensive care10,11. Patients may need to talk to a health care provider, this can be done by telehealth care services or mobile phone. The electronic medical record is vital in updating changes to medications, checking results, scheduling appointments and follow-ups. During COVID pandemic patients and healthcare workers were scared of overcrowding in clinical encounters which might increase morbidity and mortality12,13. Diabetics are prone to infections that can affect glycemic control. The recent COVID-19 pandemic coupled with the increased global burden of diabetes is becoming a challenge to the health care providers in providing effective and quality care to patients. Thus, this study was done to identify glycemic control in diabetic patients during COVID-19 pandemic.
MATERIALS AND METHODS
A retrospective cross-sectional observational study was conducted from September, 2022 to December, 2022 to fulfil the study's objectives. Clinical and laboratory parameters were extracted from the computerized databases using a predesigned questionnaire. Ethical consideration through seeking Research and Ethical Review and Approve Committee RERAC approval was done and permission to access to the electronic medical records of Falaj Al-Qabail Health Center was taken. Data was collected from the computer-based electronic data sheet without direct contact with patients so informed consent was not required. Ethical approval was taken from Ministry of Health Oman.
Data collection was done in Falaj Health Center by the co-PIs. The catchment in Falaj Al-Qabail Health Center is 30,000 populations, where on average 500 registered diabetic patients visit the health center annually.
The inclusion criteria were patients more than 18 years old registered for Diabetes at Falaj Al-Qabail Health Center from January to December, 2018. The HbA1C lab values were checked for the more than 700 registered participants for 2018, 2019, 2020 and 2021. Data on diabetic patients were collected retrospectively from the electronic medical records (Al Shifa’a 3+) using a pre-designed data collection form which includes demography, comorbidities/ complications and laboratory test result HbA1C from 2018 to 2021. The HbA1c values of 2018/2019 (pre-COVID) were compared with values from 2020/2021(post-COVID). Comparisons were made on the values to see the difference in glycemic control of registered Diabetic patients after the advent of COVID. The Dependent variable is HbA1c and the independent variables are all the sociodemographic variables, comorbidities and complications of diabetes. The data collected are anonymous without revealing the patient’s identity. The data does not include any personal or contact details of patients or relatives. Complete patient anonymity was maintained throughout the project.
Statistical analysis: The SPSS 22 was used for data analysis. Descriptive statistics in the form of mean and standard deviation were calculated to describe continuous variables. Categorical variables were described using frequency and percentages. The chi-square test was used to compare the frequency of uncontrolled and controlled diabetes covariates. Paired t-test was used for comparing mean HbA1c values pre and post-pandemic. Repeated measures ANOVA was used to get tests of within-subject effects for comparing HbA1c values across years for multiple comparisons. For this, Mauchly’s test of sphericity assumption was considered if the significance is more than 0.05. A value of <0.05 was considered for statistical significance for hypothesis testing.
RESULTS AND DISCUSSION
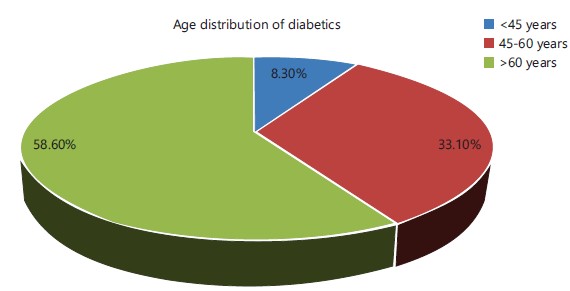
There was a total of 314 patients for whom data was collected on Diabetes from the Ministry of Health registry for diabetes in Falaj Al-Qabail Health centre. Most of the study subjects were >60 years of age (184) compared to 45 to 60 years (104) and <45 years (26) (Fig. 1).
The mean age was 62.18±12.24 years. Most of them were females (209) compared to males (105). Most (93.6%) had diabetes more than 5 years of duration. Most (92.4%) were on oral hypoglycemic agents compared to only 29.9%, who were on insulin. Mean BMI was 30.62±6.137 suggesting that most of the patients were obese. With regards to comorbidities, 76.8% had hypertension, 9.2% had ischemic heart disease, 1.6% had a stroke, 82.8% were obese, 3.8% had asthma, 1% had cancer, 7.3% had hypothyroidism and 2.5% had liver disease.
Few had complications of diabetes 35% had chronic kidney disease, 26.1% had retinopathy and 37.3% had neuropathy (Table 1). The COVID positivity was found in 14 (4.5%) patients, negative status was found in 26 (8.3%) patients and it was undocumented in most of the patients 274 (87.3%).
The HbA1c values <7% were considered controlled diabetes and more than equal to 7% was considered uncontrolled diabetes. In the current study, there were 199 (63.4%) patients with uncontrolled diabetes and 115 (36.6%) with controlled diabetes. More males had uncontrolled diabetes (64.8%) compared to females (62.7%) but this difference was not statistically significant. In patients more than 45 years of age, more uncontrolled diabetes was found (84.6%) compared to 61.5% in age less than 45 years who also had a higher percentage of controlled diabetes than patients more than 45 years of age. This difference was statistically significant, p<0.05. Patients with a duration of diabetes of more than 5 years had a higher percentage of uncontrolled diabetes (64.6%) compared to 45% in those with less duration of diabetes (p>0.05).
|
| Table 1: | Clinical characteristics of the study sample | |||
| Variable | Frequency (n = 314) |
Percentage |
| Gender | ||
| Male | 105 |
33.4 |
| Female | 209 |
66.6 |
| Age (years) | ||
| <45 | 26 |
8.3 |
| >45 | 288 |
91.7 |
| Duration of diabetes mellitus | ||
| <5 years | 20 |
6.4 |
| >5 years | 294 |
93.6 |
| Use of oral hypoglycemic agents | ||
| Yes | 290 |
92.4 |
| No | 24 |
7.6 |
| Insulin intake | ||
| Yes | 94 |
29.9 |
| No | 220 |
70.1 |
| Hypertension | ||
| Yes | 241 |
76.8 |
| No | 73 |
23.2 |
| Smoking | ||
| Yes | 9 |
2.9 |
| No | 305 |
97.1 |
| Obesity | ||
| Yes | 260 |
82.8 |
| No | 54 |
17.2 |
| Chronic kidney disease | ||
| Yes | 110 |
35 |
| No | 204 |
65 |
| Retinopathy | ||
| Yes | 82 |
26.1 |
| No | 232 |
73.9 |
| Neuropathy | ||
| Yes | 117 |
37.3 |
| No | 197 |
62.7 |
| Ischemic heart disease | ||
| Insulin | 29 |
9.2 |
| Oral | 285 |
90.8 |
| Stroke | ||
| Yes | 5 |
1.6 |
| No | 309 |
98.4 |
| Asthma | ||
| Yes | 12 |
3.8 |
| No | 302 |
96.2 |
| Hypothyroidism | ||
| Yes | 23 |
7.3 |
| No | 291 |
92.7 |
| Liver disease | ||
| Yes | 8 |
2.5 |
| No | 306 |
97.5 |
| Depression | ||
| Yes | 1 |
0.3 |
| No | 313 |
99.7 |
| Cancer | ||
| Yes | 3 |
1 |
| No | 311 |
99 |
|
Uncontrolled diabetes was seen more in patients taking insulin intake (78.7%) compared to those who did not (56.8%) and this difference was statistically significant (p<0.01). Similar differences were seen with the intake of oral hypoglycemic agents, but they were not significant. Most of the diabetic patients were hypertensive and obese irrespective of the HbA1c values. With regards to diabetes-specific complications, retinopathy was present more in uncontrolled diabetic patients (80.5%) compared to controlled diabetes (65.9%) and the difference was statistically significant (p<0.05). Similarly, uncontrolled diabetic patients had more neuropathy (70.1%) and chronic kidney disease (69.1%) compared to their controlled diabetes counterparts (p>0.05). A statistically significant difference (p<0.05) was found between liver disease patients in uncontrolled (25%) and controlled diabetes (64.4%) (Table 2).
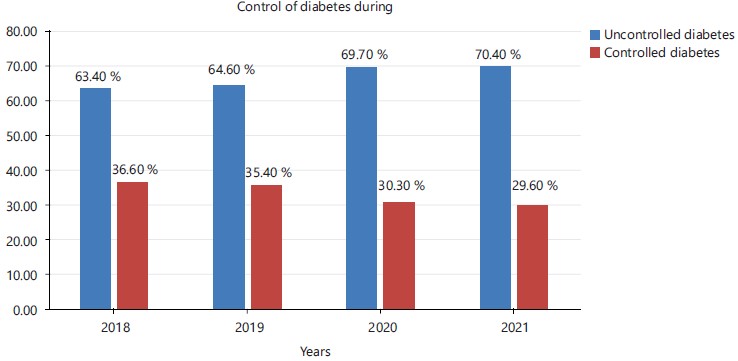
The study showed that control of diabetes worsened with the advent of COVID Uncontrolled Diabetes was 63.4% in 2018, before COVID started and subsequently increased from 2019 (64.6%) to 2020 (69.7%) to 2021 (70.4%) as shown in Fig. 2.
A paired sample t-test was conducted to determine the effect of COVID-19 on diabetes control through pre and post-pandemic HbA1c readings. The mean HbA1c from 2018-2021 is given in Table 3.
There was a significant mean difference in HbA1c readings between 2018-2020 (p<0.05) and 2019-2020, suggesting COVID-19 affected HbA1c status supporting the hypothesis of uncontrolled diabetes as shown in Table 4.
To overcome the bias in the testing of multiple pairs in paired t-test, repeated measures ANOVA test was further conducted to compare HbA1c across 2019, 2020 and 2021. Descriptive statistics are already explained in Table 3 in the form of mean and SD values of HbA1c. Mauchly’s test of sphericity assumption was met and there was no violation as χ2 (2) = 4.377, p = 0.112. Tests of within subjects’ effects showed that the difference between HbA1c across years is statistically significant; F (2, 626) = 10.155 and p = 0.000.
The interaction effect between gender and HbA1c was not significant as showing similar effects for men and women in HbA1c values across pre and post-pandemic as shown in Fig. 3.

|
| Table 2: | Attributes of uncontrolled diabetes in Oman | |||
Uncontrolled diabetes (n = 199) |
Controlled diabetes (n = 115) |
||||
| Variable | Frequency |
Percentage |
Frequency |
Percentage |
p-value |
| Gender | |||||
| Male | 68 |
64.8 |
37 |
35.2 |
0.718 |
| Female | 131 |
62.7 |
78 |
37.3 |
|
| Age (years) | |||||
| <45 | 177 |
61.5 |
111 |
38.5 |
0.019 |
| >45 | 22 |
84.6 |
4 |
15.4 |
|
| Duration of diabetes mellitus | |||||
| <5 years | 9 |
45 |
11 |
55 |
0.078 |
| >5 years | 190 |
64.6 |
104 |
35.4 |
|
| Use of oral hypoglycemic agents | |||||
| Yes | 187 |
64.5 |
103 |
35.5 |
0.157 |
| No | 12 |
50 |
12 |
50 |
|
| Insulin intake | |||||
| Yes | 74 |
78.7 |
20 |
21.3 |
0 |
| No | 125 |
56.8 |
95 |
43.2 |
|
| Hypertension | |||||
| Yes | 153 |
63.5 |
88 |
36.5 |
0.942 |
| No | 46 |
63 |
27 |
37 |
|
| Obesity | |||||
| Yes | 169 |
65 |
91 |
35 |
0.19 |
| No | 30 |
55.6 |
24 |
44.4 |
|
| Retinopathy | |||||
| Yes | 66 |
80.5 |
16 |
19.5 |
0.014 |
| No | 153 |
65.9 |
79 |
34.1 |
|
| Neuropathy | |||||
| Yes | 82 |
70.1 |
35 |
29.9 |
0.057 |
| No | 117 |
59.4 |
80 |
40.6 |
|
| Liver disease | |||||
| Yes | 2 |
25 |
6 |
75 |
0.022 |
| No | 197 |
64.4 |
109 |
35.6 |
|
| Chronic kidney disease | |||||
| Yes | 76 |
69.1 |
34 |
30.9 |
0.123 |
| No | 123 |
60.3 |
81 |
39.7 |
|
| Table 3: | Year-wise presentation of level of HbA1C | |||
| HbA1c | Mean |
SD |
| 2018 | 7.88 |
1.815 |
| 2019 | 7.808 |
1.607 |
| 2020 | 8.107 |
1.908 |
| 2021 | 8.105 |
1.85 |
| Table 4: | Paired t-test pairs of uncontrolled diabetes pre and post-COVID-19 | |||
95 (%) CI of difference |
|||||
| Pairs | Mean difference |
Lower |
Upper |
t-test |
p-value |
| 2018-2020 | 0.2274 |
0.536 |
0.4012 |
2.574 |
0.011* |
| 2019-2020 | 0.2997 |
0.1541 |
0.4453 |
4.049 |
0.000* |
| 2019-2021 | 0.2971 |
0.1381 |
0.4562 |
3.675 |
0.000* |
DISCUSSION
There were a significant number of patients with uncontrolled diabetes. More males had uncontrolled diabetes (64.8%) compared to females (62.7%) but this difference was not statistically significant. In patients more than 45 years of age, more uncontrolled diabetes was found (84.6%). Diabetes is a pandemic and a leading cause of mortality and morbidity worldwide. The COVID-19 pandemic has had a drastic effect on the healthcare system that needed service modification as there was a disruption of routine care provided to patients with diabetes mellitus (DM) in primary care. The healthcare system and patients were not prepared for this change leading to reduced physical activity, patient follow-up visits to doctors and stress related to COVID-19 infection14,15.
This study focuses on the comparison of glycemic control pre and post-COVID in diabetic patients. Regarding the gender differences more males had uncontrolled diabetes compared to females, but this difference was not statistically significant (Fig. 1). Most of the patients had diabetes of more than 5 years of duration (93.6%) and were on oral hypoglycemic agents (92.4%) compared to only 29.9%, who were on insulin. Most of the patients (82.8%) were obese (Table 1). Literature also supported the findings in the current study, the researchers reported increased stress and weight gain with relatively well-controlled type 1 and 2 diabetes during short-term lockdown measures during COVID. Literature also reported an increase in weight correlated with an increase in HbA1c and a decrease in weight correlated with a decrease in HbA1c16-18.
In this study, comorbidities were identified in more than two-thirds of patients with 76.8% having hypertension and 82.8% having obesity (Table 2 and Fig. 2). One-third of patients had diabetic nephropathy, retinopathy and neuropathy. Kalligeros et al.17 reported that hypertension and chronic kidney diseases were significantly associated with hospitalization of COVID-19 individuals.
In this study HbA1c values <7% were considered controlled diabetes and more than equal to 7% was considered uncontrolled diabetes as per Ministry guidelines. In the current study, more than two-thirds of patients had uncontrolled diabetes and one-third with controlled diabetes (Table 3 and 4). In a study from Oman, Al Harthi et al.9 reported that HbA1c decreased phone consultation, however, the evidence was not inconclusive. There was an overall increase in mean glycated hemoglobin. Khan et al.18 and Bharill et al.19 also reported similar findings from Pakistan with HBA1C as a marker of severity of COVID-19.
In this study, more uncontrolled diabetes was found (84.6%) in patients more than 45 years of age, compared to 61.5% in age less than 45 years who also had a higher percentage of controlled diabetes than patients more than 45 years of age (Fig. 3). This difference was statistically significant, p<0.05. Bharill et al.19 reported in one study that young population with T2D during the COVID-19 pandemic. Young age with T2D is at high risk for diabetes complications and worsening glycemic control20-22.
This study has shown patients with a duration of diabetes more than 5 years had a higher percentage of uncontrolled diabetes (64.6%) compared to 45% in those with less duration of diabetes (p>0.05). Uncontrolled diabetes was seen more in patients taking insulin intake (78.7%) compared to those who did not (56.8%) and this difference was statistically significant (p<0.01). Similar differences were seen with the intake of oral hypoglycemic agents, but they were not significant. Literature reported the same finding during the COVID-19 outbreak and lockdown23.
Most of the diabetic patients were hypertensive and obese irrespective of the HbA1c values. With regards to diabetes specific complications, retinopathy was present more in uncontrolled diabetic patients (80.5%) compared to controlled diabetes (65.9%) and the difference was statistically significant (p<0.05). Similarly, uncontrolled diabetic patients had more neuropathy (70.1%) and chronic kidney disease (69.1%) compared to the controlled diabetes counterpart (p>0.05). Carr et al.22 reported the indirect impact of the COVID-19 pandemic on health checks and prescribing in people with T2D marked reductions in the rate of health checks and new prescribing in people with T2D as indirect consequences of the COVID-19 pandemic22-24.
The study showed that control of diabetes worsened with the advent of COVID. There were significant mean differences in HbA1c readings between 2018-2020 (p<0.05); 2019-2020 (p<0.01) and 2019-2021 (p<0.01). This suggested COVID-19 affected HbA1c status supporting the hypothesis towards uncontrolled diabetes. A study from UK has shown that people with diabetes have been disproportionately affected by COVID-19, with growing evidence of higher mortality and morbidity25. Literature has reported geriatric age, diabetes mellitus, hypertension and obesity significantly increase the risk of hospitalization and death in COVID-19 patients26,27.
The literature reported that even in the pre-COVID period the optimum glycemic target was not fully achieved and glycemic control is still below the desired levels28. In primary care, doctors are encouraged to assess a patient-centered care model and provide orientation training29.
Literature has also shown that mortality rates were low at HbA1c 6.5 to 7.5%, with high mortality with HbA1c >9%. The importance of patient engagement, collaboration, partnership, or problem-solving, all of which may be characteristic of patient-centered approach management encourages effective outcomes and behavior change for better control of diabetes, declarations (body weight, physical activity, acute disease)29.
However, the population-representative for the country and data collected by one attending physician which excludes the influence of different views on patients’ treatment is the strength of the study. The limitation of the study is that this data is taken from only one primary care center so it cannot be generalized. This study has shown poor diabetic control during the pandemic at home so, appropriate self-care can make a significant change in diabetic control. Patients might understand the importance of self-management to control diabetes. The study is only done in one primary health care center.
CONCLUSION
Our study showed that during COVID the control of diabetes declined as evidenced from HbA1c values of 7.8 pre-COVID to 8.1 post-COVID suggesting that during COVID, patients did not get optimal care and could not visit hospitals often for advice which led to uncontrolled diabetes. Age of more than 45 years, retinopathy and insulin intake were found to be important covariates of uncontrolled diabetes (p<0.05). Even though more cases of uncontrolled diabetes were found in males, those with higher duration of diabetes and obese patients; however, these results were not statistically significant. Diabetes complications like neuropathy and chronic kidney disease also showed early markers of uncontrolled diabetes but they were not significant statistically.
SIGNIFICANCE STATEMENT
This study is done to identify glycemic control in diabetic patients during the COVID-19 pandemic. This was an observation that the diabetic patients were not attending the clinic during the pandemic however, they were taking care of their blood sugar at home. More cases of uncontrolled diabetes were found in males, those with a higher duration of diabetes and obese patients. Uncontrolled Diabetes was 63.4% in 2018 before COVID-19 started and subsequently increased from 2019 to 2021. There was a significant mean difference in HbA1c readings between 2018-2021. This study is recommended to do more studies on different primary care setups.
REFERENCES
- Shaw, J.E., R.A. Sicree and P.Z. Zimmet, 2010. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res. Clin. Pract., 87: 4-14.
- Singh, A.K., R. Gupta, A. Ghosh and A. Misra, 2020. Diabetes in COVID-19: Prevalence, pathophysiology, prognosis and practical considerations. Diabetes Metab. Syndr.: Clin. Res. Rev., 14: 303-310.
- Wang, C., P.W. Horby, F.G. Hayden and G.F. Gao, 2020. A novel coronavirus outbreak of global health concern. Lancet, 395: 470-473.
- Fadini, G.P., M.L. Morieri, E. Longato and A. Avogaro, 2020. Prevalence and impact of diabetes among people infected with SARS-CoV-2. J. Endocrinol. Invest., 43: 867-869.
- Yang, J.K., Y. Feng, M.Y. Yuan, S.Y. Yuan and H.J. Fu et al., 2006. Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabetic Med., 23: 623-628.
- Hussain, A., B. Bhowmik and N.C. do Vale Moreira, 2020. COVID-19 and diabetes: Knowledge in progress. Diabetes Res. Clin. Pract., 162.
- Al-Lawati, J.A., A.M. Al Riyami, A.J. Mohammed and P. Jousilahti, 2002. Increasing prevalence of diabetes mellitus in Oman. Diabetic Med., 19: 954-957.
- Guo, W., M. Li, Y. Dong, H. Zhou and Z. Zhang et al., 2020. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab. Res. Rev., 36.
- Al Harthi, T., H. Anwar, A. Al Lawati, F. Al Shuriqi and F. Al Rashdi et al., 2021. The impact of COVID-19 on diabetes care in muscat governorate: A retrospective cohort study in primary care. J. Primary Care Community Health, 12.
- Khamis, F., I. Al-Zakwani, H. Al Naamani, S. Al Lawati and N. Pandak et al., 2020. Clinical characteristics and outcomes of the first 63 adult patients hospitalized with COVID-19: An experience from Oman. J. Infect. Public Health, 13: 906-913.
- Fang, L., G. Karakiulakis and M. Roth, 2020. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med., 8.
- Gupta, R., A. Ghosh, A.K. Singh and A. Misra, 2020. Clinical considerations for patients with diabetes in times of COVID-19 epidemic. Diabetes Metab. Syndr.: Clin. Res. Rev., 14: 211-212.
- Huang, I., M.A. Lim and R. Pranata, 2020. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia-A systematic review, meta-analysis, and meta-regression. Diabetes Metab. Syndr.: Clin. Res. Rev., 14: 395-403.
- Tewari, A., V. Tewari and J. Tewari, 2021. Effect of COVID 19 lockdown on glycemic parameters in people with type 2 diabetes. J. Fam. Med. Primary Care, 10: 2529-2532.
- Ruissen, M.M., H. Regeer, C.P. Landstra, M. Schroijen and I. Jazet et al., 2021. Increased stress, weight gain and less exercise in relation to glycemic control in people with type 1 and type 2 diabetes during the COVID-19 pandemic. BMJ Open Diabetes Res. Care, 9.
- Wysocki, M., M. Walędziak, M. Proczko-Stepaniak, M. Pędziwiatr, J. Szeliga and P. Major, 2021. Lifestyle changes in patients with morbid obesity and type 2 diabetes mellitus during the COVID-19 pandemic. Diabetes Metab., 47.
- Kalligeros, M., F. Shehadeh, E.K. Mylona, G. Benitez, C.G. Beckwith, P.A. Chan and E. Mylonakis, 2020. Association of obesity with disease severity among patients with coronavirus disease 2019. Obesity, 28: 1200-1204.
- Khan, R., S. Khan, Z. Khan, A.U. Khan and A. Mahmood et al., 2022. Higher pre-infection HbA1c level in diabetic individuals as a marker of severity of COVID-19. Pak. J. Med. Health Sci., 16: 981-983.
- Bharill, S., T. Lin, A. Arking, E.A. Brown and M. West et al., 2022. Worsening glycemic control in youth with type 2 diabetes during COVID-19. Front. Clin. Diabetes Healthcare, 3.
- Eberle, C. and S. Stichling, 2021. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: A systematic review. Diabetology Metab. Syndr., 13.
- Khare, J. and S. Jindal, 2020. Observational study on effect of lock down due to COVID 19 on glycemic control in patients with diabetes: Experience from Central India. Diabetes Metab. Syndr.: Clin. Res. Rev., 14: 1571-1574.
- Carr, M.J., A.K. Wright, L. Leelarathna, H. Thabit and N. Milne et al., 2022. Impact of COVID-19 restrictions on diabetes health checks and prescribing for people with type 2 diabetes: A UK-wide cohort study involving 618 161 people in primary care. BMJ Qual. Saf., 31: 503-514.
- Taher, N., M.S.B. Huda and T.A. Chowdhury, 2020. COVID-19 and diabetes: What have we learned so far? Clin. Med., 20: e87-e90.
- Muniyappa, R. and S. Gubbi, 2020. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am. J. Physiol.-Endocrinol. Metab., 318: E736-E741.
- Sutkowska, E., D.M. Marciniak, K. Sutkowska, K. Biernat, J. Mazurek and N. Kuciel, 2022. The impact of lockdown caused by the COVID-19 pandemic on glycemic control in patients with diabetes. Endocrine, 76: 273-281.
- Alawadi, F., E. Abdelgadir, A. Bashier, M. Hassanein and F. Rashid et al., 2019. Glycemic control in patients with diabetes across primary and tertiary government health sectors in the Emirate of Dubai, United Arab Emirates: A five-year pattern. Oman Med. J., 34: 20-25.
- Al Mahrouqi, A.S., R.K. Mallinson, K.M. Oh and A.A. Weinstein, 2022. Patients’ and nurses’ perceptions of diabetes self-management in Oman: A qualitative study. Int. J. Environ. Res. Public Health, 19.
- Al-Ghamdi, S.M.G., B. Bieber, M. Al Rukhaimi, A. Al Sahow and I. Al Salmi et al., 2022. Diabetes prevalence, treatment, control, and outcomes among hemodialysis patients in the gulf cooperation council countries. Kidney Int. Rep., 7: 1093-1102.
- Tanji, Y., S. Sawada, T. Watanabe, T. Mita and Y. Kobayashi et al., 2021. Impact of COVID-19 pandemic on glycemic control among outpatients with type 2 diabetes in Japan: A hospital-based survey from a country without lockdown. Diabetes Res. Clin. Pract., 176.
How to Cite this paper?
APA-7 Style
Jahan,
F., Anwar,
S., Al Shibli,
I.F., Al Saadi,
B.K., Al Ghaithi,
A.A., Al Mamari,
I.H. (2023). Glycemic Control in Diabetic Patients During COVID-19 Pandemic, A Study from North Al-Batinah, Oman. Trends in Medical Research, 18(1), 187-196. https://doi.org/10.3923/tmr.2023.187.196
ACS Style
Jahan,
F.; Anwar,
S.; Al Shibli,
I.F.; Al Saadi,
B.K.; Al Ghaithi,
A.A.; Al Mamari,
I.H. Glycemic Control in Diabetic Patients During COVID-19 Pandemic, A Study from North Al-Batinah, Oman. Trends Med. Res 2023, 18, 187-196. https://doi.org/10.3923/tmr.2023.187.196
AMA Style
Jahan
F, Anwar
S, Al Shibli
IF, Al Saadi
BK, Al Ghaithi
AA, Al Mamari
IH. Glycemic Control in Diabetic Patients During COVID-19 Pandemic, A Study from North Al-Batinah, Oman. Trends in Medical Research. 2023; 18(1): 187-196. https://doi.org/10.3923/tmr.2023.187.196
Chicago/Turabian Style
Jahan, Firdous, Sanam Anwar, Ibrahim Fadhil Al Shibli, Buthaina Khalifa Al Saadi, Asil Asim Al Ghaithi, and Iman Hamdan Al Mamari.
2023. "Glycemic Control in Diabetic Patients During COVID-19 Pandemic, A Study from North Al-Batinah, Oman" Trends in Medical Research 18, no. 1: 187-196. https://doi.org/10.3923/tmr.2023.187.196

This work is licensed under a Creative Commons Attribution 4.0 International License.